As many of you know, under the current administration of Governor Jan
Brewer the suicide and homicide rates among state prisoners doubled
almost immediately. Those rates have persisted while the level of violence and despair have escalated over the course of the past four
years under the directorship of Arizona Department of Corrections' Charles Ryan.
Conditions and access to medical care in Arizona's state prisons had so deteriorated under Ryan that the ACLU and Prison Law
Office, among others, filed a suit against him and AZ DOC Health Services Director
Richard Pratt last year on behalf of 14 state prisoners, with plans to make it a class action involving every state prisoner. The abuse of solitary confinement in managing mentally ill prisoners was a central feature of the suit as well.
On March 6, 2013, "Parsons v Ryan" was finally certified as a CLASS ACTION.
Thank
you not only to all the legal staff who brought it this far, but also
to Wendy Halloran, KPNX, and the families who have survived the horrors
of prison violence in this state with a resolve to make sure that the
gross indifference to human life at the AZ DOC kills no more....here's
the story on Channel 12/KPNX when the suit was first filed:
----------------------
ORIGINAL POST (2/5/13) Suing Arizona:
Parsons v. Ryan should be a class action...
Below the mural remembering state prisoners who died from
deliberate indifference, suicide, or other violence under Jan Brewer's
administration is the full text of the Parsons v Ryan complaint seeking
class action status to sue the AZ Department of Corrections Director and
Health Services Director over gross medical, dental and psychiatric
neglect, and the abuse of solitary confinement to manage prisoners with
mental illness. We are still awaiting Judge Neil Wake's decision on the motion for class designation so the case can proceed as a class action suit.
These are just a few of the nearly 70 names of the AZ Department of Corrections' wrongfully-dead, remembered on the sidewalk outside of the Sandra Day O'Connor Federal Courthouse in Phoenix (January 25, 2013) - thanks to all who came out to help.
These were not isolated incidents, by the way, Judge Wake. Under Chuck Ryan, the homicide and suicide rates have both doubled, the assault rate has tripled, and the incidence of gross medical neglect and outright abuse suggest pervasive, system-wide problems affecting potentially every prisoner. The scale of constitutional violations by the AZ DOC (and now Wexford Health Sources) is staggering. I don't know how this case could be anything BUT a class action...








Ophelia Venegas, remembering her only son, Joseph, who died last year
in Yuma Prison of pneumonia. He was only 29.
And here is Parson v Ryan: this should enrage anyone out there with a soul. We must begin to
treat people better than this if we ever hope to curb the level of
violence and victimization in this country...
----PARSONS v RYAN (March 22, 2012)--
Daniel
J. Pochoda (SBA 021979)
James
Duff Lyall (SBA 330045)*
ACLU
FOUNDATION OF ARIZONA
3707
N. 7th Street, Suite 235
Phoenix,
AZ 85013
Telephone:
(602) 650-1854
dpochoda@acluaz.org
jlyall@acluaz.org
*Admitted
pursuant to Ariz. Sup. Ct. R. 38(f)
Attorneys
for Plaintiffs Robert Gamez, Shawn Jensen, Stephen Swartz, Dustin
Brislan, Sonia Rodriguez, Christina Verduzco, Jackie Thomas, Jeremy
Smith, Victor Parsons, Maryanne Chisholm, Desiree Licci, Joseph
Hefner, Joshua Polson, and Charlotte Wells, on behalf of themselves
and all others similarly situated
[ADDITIONAL
COUNSEL LISTED ON SIGNATURE PAGE]
Jennifer
Alewelt (SBA 027366)
Ruth
Szanto (SBA 029073)
ARIZONA
CENTER FOR DISABILITY LAW
5025
East Washington St. Suite 202
Phoenix,
AZ 85034
Telephone
(602) 274-6287
jalewelt@azdisabilitylaw.org
rszanto@azdisabilitylaw.org
Attorneys
for Plaintiff Arizona Center for Disability Law
UNITED
STATES DISTRICT COURT DISTRICT OF ARIZONA
Victor
Parsons; Shawn Jensen; Stephen Swartz; Dustin Brislan; Sonia
Rodriguez; Christina Verduzco; Jackie Thomas; Jeremy Smith; Robert
Gamez; Maryanne Chisholm; Desiree Licci; Joseph Hefner; Joshua
Polson; and Charlotte Wells, on behalf of themselves and all others
similarly situated; and Arizona Center for Disability Law,
Plaintiffs,
v.
Charles
Ryan, Director, Arizona Department of Corrections; and Richard Pratt,
Interim Division Director, Division of Health Services, Arizona
Department of Corrections, in their official capacities,
Defendants
No.
CLASS
ACTION
CLASS
ACTION COMPLAINT FOR INJUNCTIVE AND DECLARATORY RELIEF
NATURE
OF THE ACTION
1.
Prisoner Plaintiffs and the Plaintiff Class are housed in Arizona
Department of Corrections (“ADC”) state prisons, and seek
declaratory and injunctive relief against Charles Ryan and Michael
Pratt, (collectively, “Defendants”) in their official capacities.
Prisoner Plaintiffs and the Plaintiff Class are entirely dependent on
Defendants for their basic health care. However, the system under
which Defendants Ryan and Pratt provide medical, mental health, and
dental care (collectively, “health care”) to prisoners is grossly
inadequate and subjects all prisoners to a substantial risk of
serious harm, including unnecessary pain and suffering, preventable
injury, amputation, disfigurement, and death. For years, the health
care provided by Defendants in Arizona’s prisons has fallen short
of minimum constitutional requirements and failed to meet prisoners’
basic health needs. Critically ill prisoners have begged prison
officials for treatment, only to be told “be patient,” “it’s
all in your head,” or “pray” to be cured. Despite warnings from
their own employees, prisoners and their family members, and
advocates about the risk of serious injury and death to prisoners,
Defendants are deliberately indifferent to the substantial risk of
pain and suffering to prisoners, including deaths, which occur due to
Defendants’ failure to provide minimally adequate health care, in
violation of the Eighth Amendment. “Just as a prisoner may starve
if not fed, he or she may suffer or die if not provided adequate
medical care. A prison that deprives prisoners of basic sustenance,
including adequate medical care, is incompatible with the concept of
human dignity and has no place in civilized society.” Brown v.
Plata, 563 U.S. __, 131 S.Ct. 1910, 1928 (2011).
2.
Arizona prisoners also suffer serious harm and are subject to a
substantial risk of serious harm as a result of Defendants holding
prisoners in isolation in supermax Special Management Units (“SMUs”)
in cruel and unusual conditions of confinement. Defendants continue
to be deliberately indifferent to the substantial risk of pain and
suffering, including deaths, which occur due to their systemic
failure to provide minimally adequate conditions to prisoners in
isolation, in violation of the Eighth Amendment. 3. Plaintiffs seek
injunctive relief to compel Defendants to immediately provide
prisoner-Plaintiffs and the class members they represent with
constitutionally adequate health care and with protection from
unconstitutional conditions of confinement.
JURISDICTION
4.
This Court has jurisdiction pursuant to 28 U.S.C. §§ 1331 and 1343.
This civil action seeks declaratory and injunctive relief under 28
U.S.C. §§1343, 2201, and 2202; and 42 U.S.C. § 1983.
VENUE
5.
Venue is proper under 28 U.S.C. § 1391(b), because the Defendants
reside in the District of Arizona, and because a substantial part or
all of the events or omissions giving rise to Plaintiffs’ claims
occurred in the District of Arizona.
PARTIES
6.
Plaintiff Victor Parsons is a prisoner in ADC’s Lewis complex. Mr.
Parsons has been diagnosed with Attention Deficit Hyperactivity
Disorder (ADHD) with a possible history of bipolar disorder. Mr.
Parsons has received inadequate mental health care, including abrupt
stopping and starting of medication, inappropriate medication, and
delays in follow up appointments. For example, in June 2010, Mr.
Parsons’ medications were suddenly discontinued without
explanation. After he began to decompensate and experience
psychiatric symptoms, he submitted an HNR requesting treatment. Mr.
Parsons’ medication was abruptly restarted without titrating,
placing him at high risk for severe side effects. Mr. Parsons has
also experienced delays in his dental care. Mr. Parsons filed four
HNRs in 2009 complaining that a temporary filling had fallen out of
his tooth. Each time he was seen, Parsons was given another temporary
filling that would fall out weeks later, forcing him to restart the
process. He was told that the only alternative was to have his tooth
pulled, but he refused. After five months, he finally received a
permanent filling.
7.
Plaintiff Shawn Jensen is a prisoner in ADC’s Tucson complex.
Defendants have failed to provide him with adequate and timely
medical care, causing him harm and permanent injury. Mr. Jensen has a
history of prostate cancer. In ADC custody, he encountered delays in
having the cancer diagnosed and treated and continues to experience
harm and injuries caused by Defendants’ inadequate medical care. In
November 2006, Mr. Jensen was tested with a Prostate Antigen (PSA)
Test and found to have an elevated score of 8.4 and a nodule on the
prostate. Once the PSA is over 7, most clinicians order a biopsy. A
prison doctor referred him for a biopsy in January 2007, but he did
not receive the biopsy until October 2009, after his PSA score had
risen to 9.3. The biopsy revealed he had Stage 2 prostate cancer, an
aggressive form, and by February 2010 his PSA score was 12 and
urologists recommended aggressive treatment of the cancer, a bone
scan to determine the extent of the cancer, and surgery to remove the
tumor. Mr. Jensen experienced gaps as long as two months in getting
from the prison pharmacy the chemotherapy medication that was
prescribed for him by outside urologists. He did not have the surgery
until mid-July 2010. When he returned to prison after the surgery,
Defendants provided incompetent medical care, and Mr. Jensen suffered
harm and permanent injuries due to staff performing medical
procedures for which they were not qualified.
8.
Plaintiff Stephen Swartz is a prisoner in ADC’s Lewis complex. In
February 2010, Mr. Swartz suffered eye injuries and extensive facial
fractures as a result of an inmate assault. He did not receive timely
follow-up with a plastic surgeon or ophthalmologist, but was instead
referred to an oral surgeon to treat the facial fractures. Despite
multiple referrals from prison doctors for specialty care, Mr. Swartz
did not see an ophthalmologist until January 2011, almost a year
after he was assaulted, and has permanent partial paralysis to his
face. Mr. Swartz filed numerous HNRs to address untreated neuropathic
pain, and repeatedly waited months to learn whether pain medications
would be approved and provided. He continues to report chronic pain.
Mr. Swartz is also diagnosed with bipolar disorder and major
depressive disorder, and despite multiple incidents of self-harm, has
received inadequate mental health care while on suicide watch and in
isolation in a SMU. Additionally, Mr. Swartz has had a cracked molar
for two years. When he went to the dentist for the pain, Mr. Swartz
was refused a filling and told the only available treatment was to
pull the tooth.
9.
Plaintiff Dustin Brislan is a prisoner in ADC’s Eyman complex,
housed in a SMU. Mr. Brislan is diagnosed with bipolar disorder,
schizoaffective disorder, and borderline personality disorder, and he
has a designation of Serious Mental Illness (“SMI”). He engages
in severe self-injurious behavior – including cutting, head
banging, and self-starvation. As a result of his mental illness, he
experiences depression, hallucinations, suicidal ideation, and
paranoia. Despite the severity of Mr. Brislan’s condition,
Defendants have failed to provide him with minimally adequate mental
health care. Mr. Brislan has received improper medication, and has
experienced delays in receiving and abrupt changes to his medication.
Mr. Brislan has not been monitored regularly by a psychiatrist, or
received therapeutic treatment to address his extreme self-harming
behavior. Instead, he has been placed on suicide watch for excessive
lengths of time, where he did not receive adequate treatment and
continued to commit repeated acts of self-harm.
10.
Plaintiff Sonia Rodriguez is a prisoner in ADC’s Perryville
complex. She is designated as SMI, and she experiences depression,
anxiety, and hallucinations. Defendants have failed to provide Ms.
Rodriguez with minimally adequate mental health care, and she has
experienced poor medication management, lack of therapeutic
treatment, and conditions of cruel and inhumane confinement in
Perryville’s SMU and on suicide watch. The harsh conditions and
extreme isolation of the SMU and on suicide watch have worsened her
mental conditions. Ms. Rodriguez has asthma, and has experienced
multiple asthma attacks and breathing problems due to the ongoing use
of pepper spray by correctional staff on the women housed in the SMU
and in suicide watch. On multiple occasions, her medications have
been abruptly discontinued or changed and her dosage adjusted without
explanation or proper monitoring. As a result, Ms. Rodriguez has
suffered severe side effects, including uncontrolled shaking,
difficulty speaking, and physical “slowing” and lethargy, and a
worsening of her mental health symptoms.
11.
Plaintiff Christina Verduzco is a prisoner in ADC’s Perryville
complex, housed in a SMU. Ms. Verduzco is diagnosed with paranoid
schizophrenia, bipolar disorder, and borderline personality disorder.
She experiences a variety of symptoms, including auditory and visual
hallucinations, anxiety, paranoia, and self-harm by cutting herself.
Defendants have failed to provide her with minimally adequate mental
health care. She is confined in isolation in Perryville’s SMU and
has been placed on suicide watch on multiple occasions, most recently
in February 2012. While on suicide watch, Ms. Verduzco is forced to
wear a smock that barely comes to the top of her thighs, such that
her legs and arms are exposed to cold air. While on suicide watch,
she has no way to turn out the lights, which are sometimes left on 24
hours a day, and she is subjected to safety checks every 10 to 30
minutes, where correctional staff wake her up if she is asleep. As a
result, she cannot sleep, which aggravates her condition. Ms.
Verduzco has minimal human contact, cannot go outside, brush her
teeth, or bathe regularly. Outside of suicide watch in the SMU, her
experience is similar: extended isolation, limited exercise, and
limited therapeutic treatment. Ms. Verduzco has asthma, but she has
been pepper sprayed repeatedly by corrections officers. After being
sprayed, she has been dragged out of her cell, hosed down, and thrown
back into her cell. Ms. Verduzco has been pepper sprayed so much and
so often that she now says she is developing a tolerance to the
spray.
12.
Plaintiff Jackie Thomas is a prisoner in ADC’s Eyman complex,
housed in a SMU. Mr. Thomas has been diagnosed with depression and
seizure disorders. Although Mr. Thomas did not have suicidal ideation
when he first arrived at the SMU, his mental and medical conditions
have deteriorated over time as he has experienced prolonged periods
of isolation in the SMU. While isolated in the SMU, he has become
suicidal and committed multiple acts of self-harm, has developed
insomnia and lost a great deal of weight. As a result, he has been
placed in suicide watch multiple times, where he received minimal
mental health care. Mr. Thomas has experienced multiple failures in
the administration of his mental health care, including improper
cessation and initiation of psychotropic medications, failure to
administer prescribed medication, repeated use of ineffective
medications and medications with severe side effects, lack of
informed consent, and long delays in follow up and psychiatric
evaluation. In November 2011, Mr. Thomas overdosed on Diclofenac and
did not receive medical attention.
13.
Plaintiff Jeremy Smith is a prisoner in ADC’s Eyman complex, housed
in a SMU. Mr. Smith is diagnosed with depression, a condition
aggravated by interruptions in his mental health treatment and his
prolonged and indefinite incarceration in the SMU. Mr. Smith’s
medications have been abruptly discontinued without explanation and
restarted at inappropriate times, after lengthy delays, and without
proper evaluation by a psychiatrist. Mr. Smith also has been
prescribed powerful medications not indicated for depression. For
example, beginning in April 2008, Mr. Smith was given a potent
antipsychotic medication carrying a risk of severe side effects,
without first being seen by the doctor. His file contains no
documentation as to why that medication was prescribed or any
indication that Mr. Smith gave his informed consent to receive it.
The impact of Mr. Smith’s improper care is compounded by the
extreme isolation he experiences in the SMU. Mr. Smith has formally
renounced his former gang membership (“debriefed”) and is thus
eligible to be placed in a less restrictive setting; however, despite
his mental health condition ADC refuses to transfer him out of the
SMU.
14.
Plaintiff Robert Gamez is a prisoner in ADC’s Eyman complex, housed
in a SMU. Mr. Gamez suffered a childhood head injury and has been
diagnosed with borderline IQ, possible Post-Traumatic Stress Disorder
(PTSD), and possible frontal lobe dysfunction, symptoms of which
include major depression, panic and anxiety. Although Mr. Gamez
displays symptoms consistent with frontal lobe dysfunction and an
initial screen was positive, ADC never conducted follow up tests to
confirm his diagnosis. Mr. Gamez has experienced multiple
interruptions in care, including delays in responses to his Health
Needs Requests (“HNRs”), delays in receiving and abrupt changes
to his medication, receiving improper medication, inadequate
monitoring and follow up visits, and a lack of psychological services
for pronounced mental health deterioration during his prolonged
isolation in the SMU. For example, beginning in August 2009, Mr.
Gamez submitted multiple HNRs describing symptoms of paranoia,
anxiety, panic, and psychosis, and asking to be taken off his
medications and out of isolation. Despite experiencing acute
symptoms, Mr. Gamez was not seen for five months. Mr. Gamez’s care
was managed by a nurse practitioner, and he was not seen by a
psychiatrist from 2007 to 2011 despite referrals from staff, multiple
HNRs and deteriorating mental and physical health.
15.
Plaintiff Maryanne Chisholm is a prisoner in ADC’s Perryville
complex. Ms. Chisholm has been diagnosed with hypertension, but was
not referred to a cardiologist for eight months, despite experiencing
chest pains and shortness of breath. Ms. Chisholm has been diagnosed
with bipolar disorder, Obsessive Compulsive Disorder, and depressive
disorder. She has experienced significant delays and interruptions in
medication delivery and psychiatric care and follow-up, which have
contributed to worsening symptoms. In April 2011, Ms. Chisholm
reported experiencing a nervous breakdown and requested an adjustment
of medication; however, she was not seen by a psychiatrist for one
month and did not receive a follow up appointment as scheduled. Ms.
Chisholm’s mental health has also been adversely impacted by
custodial harassment. Shortly after first meeting with Plaintiffs’
counsel in October 2011, Ms. Chisholm was subjected to three
aggressive room searches in as many weeks. When she asked for an
explanation Ms. Chisholm was told that she was “causing problems.”
In February 2012, staff again searched her cell three separate times,
and confiscated a book of art and her art supplies, which Ms.
Chisholm relies on to manage her mental health symptoms. The art
supplies were taken because she had painted a shelf in her cell
without permission – in 2008. She also has a broken tooth and
another tooth with a missing crown. The dentist told her the only
available treatment was to pull her teeth, which she has refused.
16.
Plaintiff Desiree Licci is an inmate in ADC’s Perryville complex.
Ms. Licci has a family history of cancer and was herself treated for
cancer ten years ago. In 2010 she observed multiple masses growing on
her breasts, mouth, and arms, and reported discomfort in her cervix.
Starting in December 2010, Ms. Licci requested testing, and in April
2011 the prison doctor referred her to an oncologist. However, she
has still not seen an oncologist and was not sent for a CT scan until
September 2011. In the interim, Ms. Licci began experiencing frequent
diarrhea, nausea, exhaustion, weight loss, pain, and other alarming
symptoms. The CT scan detected multiple masses in Ms. Licci’s
reproductive organs and biopsies and a colonoscopy were ordered.
Still, the Perryville gynecologist insisted that nothing was wrong
with her reproductive organs. Ms. Licci did not receive an MRI until
December 2011, and it was not properly administered. Ms. Licci had to
submit a grievance and wait another month before receiving a second
MRI, which confirmed multiple masses on both ovaries. In January
2012, Ms. Licci asked the Perryville Facility Health Administrator
(FHA) why she still had not seen an oncologist approximately eight
months after being referred by the prison doctor. The FHA told Ms.
Licci the oncologist refused to see her without her complete file and
that ADC “didn’t have” Volume I of her file. However, ADC has
Ms. Licci’s complete file, as it was produced to Plaintiffs’
counsel in January 2012. Additionally, Ms. Licci has a Port-a-cath
implanted in her chest; however, nothing in her file indicates
whether or not it was properly flushed by medical staff prior to
November 2011.
17.
Plaintiff Joseph Hefner is a prisoner in ADC’s Lewis complex. Mr.
Hefner has impaired vision and experiences eye pain as a result of
Defendants’ failure to provide him with minimally adequate health
care. In 2006, Mr. Hefner’s vision deteriorated rapidly after an
ADC nurse gave him expired eye drops. In 2006, and again in 2008, Mr.
Hefner did not timely receive doctor-prescribed eye medication
following eye surgery. Although he has submitted numerous HNRs for
recurrent eye pain and twice been referred by an optometrist to see
an ophthalmologist, Mr. Hefner has been waiting to see an
ophthalmologist for over three years. In March 2011, Mr. Hefner was
hospitalized for injuries sustained in a prison altercation. His
outside medical records were not requested by the prison physician
until three months later, after Mr. Hefner submitted multiple HNRs
describing persistent pain and requesting treatment. The records were
never reviewed. A CT scan was not done until October 2011, seven
months after Mr. Hefner’s injury. Mr. Hefner also has chronic
gastroesophageal reflux disease (GERD) but his requests for a medical
diet have been denied.
18.
Plaintiff Joshua Polson is a prisoner in ADC’s Eyman complex,
housed in a SMU. Mr. Polson has been diagnosed with bipolar disorder,
mood disorder, and psychosis. He experiences mood swings,
hallucinations, paranoia, and depression, all of which are caused or
worsened as a result of Defendants’ failure to provide him with
minimally adequate mental health care. Mr. Polson has a family
history of suicide and he has attempted suicide three times.
Nonetheless, he is incarcerated in isolation, where he has minimal
human contact, which results in increased suicidal ideation. He has
experienced repeated gaps in his medication and sporadic monitoring
of his medication levels. Additionally, Mr. Polson experiences
chronic ear infections and has permanent hearing loss in his right
ear following significant delays in care, including delays in seeing
a physician, delays in follow-up appointments, and delays in
referrals to outside specialists. After losing hearing in his right
ear, Mr. Polson submitted multiple HNRs for chronic pain in his left
ear, but was not evaluated by a doctor for over a month. Mr. Polson
also experienced multiple problems with his dental care. He had long
delays in treatment for teeth that were broken, and waited three
years to receive partial dentures for many missing teeth. Mr. Polson
filed a request to see the dentist about a front tooth that had
broken off and was causing him a great deal of pain. He was told in
response that he was requesting routine care, and he had to wait five
months to see the dentist. The remaining portion of the tooth was not
extracted until a year after it broke off.
19.
Plaintiff Charlotte Wells is a prisoner in ADC’s Perryville
complex. Ms. Wells has a history of heart disease and high blood
pressure, and suffered a heart attack prior to being incarcerated.
She arrived to ADC custody in October 2009 complaining of chronic
chest pains, and continued to experience dizziness and high blood
pressure but was not evaluated by a cardiologist until she was
hospitalized four months later for a blocked artery. Ms. Wells
received a stent, but two days after returning to Perryville she
again reported chest pains. Ms. Wells was not seen by a doctor or
returned to the hospital, despite her history and the high risk of
arterial clogging and heart attack immediately following the
placement of a stent. She experienced chest pain and high blood
pressure, for which she was repeatedly evaluated not by an outside
cardiologist but rather by the Perryville gynecologist. Ms. Wells
continues to have problems with her blood pressure and intermittent
chest pain. Additionally, Ms. Wells experienced broken fillings in
two of her teeth in 2010. She complained of pain and requested the
fillings be repaired, but was told the only option was to have the
teeth pulled, or submit a HNR and wait months to have the fillings
approved. She did this, and endured pain for several months before
her filings were replaced; however, when she got the filling, the
dentist cracked an adjacent tooth. Again, she was told she could have
the tooth pulled, or to submit another HNR and wait for a filling.
She has waited since November 2011 for repair to the damaged tooth.
20.
Plaintiff Arizona Center for Disability Law (“ACDL”) is
designated as Arizona’s authorized protection and advocacy agency
under the Protection and Advocacy for Individuals with Mental Illness
Act (“PAIMI”), 42 U.S.C. § 10801, et. seq. ACDL has statutory
authority to pursue legal, administrative, and other appropriate
remedies to ensure the protection of individuals with mental illness
who are or will be receiving care and treatment in the State of
Arizona. 42 U.S.C. § 10805(a)(1). ACDL is pursuing this action to
protect and advocate for the rights and interests of prisoners who
are “individuals with mental illness” as that term is defined in
42 U.S.C. § 10802. The interests that ACDL seeks to vindicate by
bringing this lawsuit – the protection of the rights of individuals
with mental illness – are central to ACDL’s purpose.
21.
Defendant Charles Ryan is the Director of the ADC, and he is sued
herein in his official capacity. As the Director of the ADC, Mr. Ryan
is responsible for establishing, monitoring, and enforcing overall
operations, policies, and practices of the Arizona state prison
system, which includes the provision of constitutionally adequate
medical, mental health, and dental care for all prisoners committed
to the custody of ADC. A.R.S. §§ 31-201, 41-1604 (A), 41-1608. As
Director, Mr. Ryan is responsible for decisions concerning staff
hiring, supervision, deployment, and training that directly affect
prisoners’ abilities to obtain adequate and necessary health
services. He is responsible for providing constitutional conditions
of confinement in all units, including but not limited to isolation
units. At all times relevant hereto, he has acted under color of
state law.
22.
Defendant Richard Pratt, P.A.,1 is the Interim Division Director of
the Health Services Division of the ADC and is sued in his official
capacity. As Division Director, Mr. Pratt is responsible for
establishing, monitoring, and enforcing system-wide health care
policies and practices. He is responsible for supervising the
provision of adequate medical, mental health, and dental care for all
prisoners within the custody of the department, including but not
limited to isolation units. At all times relevant hereto, he has
acted under color of state law.
FACTUAL
ALLEGATIONS
1
Mr. Pratt’s Physician Assistant license (#2342) with the Arizona
Regulatory Board of Physician Assistants expired on Oct. 1, 2004 and
has not been renewed as of the date of this filing. Mr. Pratt
recently replaced Michael Adu-Tutu, D.D.S., as Division Director of
Health Services. Plaintiffs’ allegations refer to Defendant Pratt
because he is the current Division Director, and notwithstanding that
the majority of acts and omissions described herein occurred during
the tenure of Mr. Pratt’s predecessor, Dr. Adu-Tutu.
23.
Defendants promise prisoners through written policies to provide
sufficient resources to provide the “community standard of health
care,” but fall far below that measure. ADC Dept. Order 1101.01,
1.1. Defendants’ written policies are more honored in the breach
than in the observance, leaving prisoners at the mercy of de facto
policies that put their lives and health at risk.2 Defendants are
well aware of severe system-wide deficiencies that have caused and
continue to cause significant harm to the prisoners in their custody,
yet they have failed to take reasonable measures to abate the
impermissible risk of harm. In recent years, Defendants ignored
repeated warnings of the inadequacies of the health care system and
of the dangerous conditions in their isolation units that they
received from inmate grievances, reports from outside groups, and
complaints from prison personnel, including their own staff. For
example, in December 2009, a prison physician emailed Defendant Ryan
complaining that ADC officials were breaking the law by not providing
adequate health care. James Baird, M.D., the Director of Medical
Services, responded on behalf of Defendant Ryan and stated, “[t]he
Department has not been found, as yet, to be deliberately
indifferent. … Is the Department being deliberately indifferent?
Maybe. Probably. That would be up to a Federal Judge to decide. I do
think that there would be numerous experts in the field that would
opine that deliberate indifference has occurred.”
24.
The Deputy Medical Director for Psychiatry at the Eyman prison warned
Defendant Ryan and Defendant Pratt’s predecessor as Health Services
Director, Michael
2
As used hereafter, “policy and practice” includes unwritten
policies, customs, and actual practices of Defendants. Adu-Tutu,
D.D.S., in a series of emails in the fall of 2009 that prisoners “are
not receiving a reasonable level of psychiatric care. We are out of
compliance with our own policies regarding minimum frequency of
contact with a provider, as well as community standards for adequate
care. The lack of treatment represents an escalating danger to the
community, the staff and the inmates.”
25.
On October 12, 2011, counsel for Plaintiffs submitted a 21-page
demand letter to Defendant Ryan, describing numerous systemic
problems in the health care system and isolation units operated by
Defendants, and detailing multiple examples of harm and injuries to
prisoners resulting from these inadequate policies and practices.
Defendant Ryan initially responded by requesting three months to
investigate these problems. In the subsequent months, counsel for
Plaintiffs continued to notify Defendants of individual prisoners
asking for immediate attention to health care problems. However, as
of this date, Defendant Ryan has not provided any substantive
response to the issues raised in the letter other than to say that he
did not think the ADC health care system had any systemic problems.
I.
Defendants Deprive Plaintiffs of Constitutionally Adequate Health
Care in Violation of the Eighth Amendment
26.
Plaintiffs and the Plaintiff class allege the following. Defendants
Ryan and Pratt have a policy and practice of failing to provide
prisoners with adequate health care, and are deliberately indifferent
to the fact that the systemic failure to do so results in significant
injury and a substantial risk of serious harm.
A.
Prisoners Face Lengthy and Dangerous Delays in Receiving and Outright
Denials of Health Care
27.
Defendants have a policy and practice of failing to provide timely
access to health care and are deliberately indifferent to the risk of
harm and injury to prisoners that results from this systemic failure.
To request health care, prisoners must submit a HNR form, describing
the need for medical, dental, or mental health attention, regardless
of whether they have informed medical staff about their symptoms.
Prisoners face numerous barriers in submitting this required form:
oftentimes, there are no HNR forms in living units; staff give
prisoners photocopies of HNR forms that are later rejected for not
being originals; correctional officers refuse to provide forms to
prisoners or discourage them from filing them; and officers read
completed HNRs and tell prisoners they are not sick, and refuse to
accept or forward the HNR to health care personnel.
28.
In addition, officers sometimes prohibit prisoners from assisting
fellow inmates in completing HNRs, even though the officers are aware
that this prevents some prisoners from filing requests. This
prohibition also harms prisoners who are acutely ill, experiencing
severe mental health problems, vision-impaired, developmentally
disabled, illiterate, have injuries or permanent disabilities that
make it difficult to write, or are otherwise unable to fill out the
forms, especially because staff members will not provide assistance.
For example, Plaintiff Smith has an injury to his hand that prevents
him from writing. He asked officers to assist him in completing the
HNRs, but the officers stated they were prohibited by ADC policy from
helping him.
29.
In addition to restricting the ability of prisoners to request health
care, Defendants have a policy and practice of failing to provide
care after receiving notice of prisoners’ needs, and are
deliberately indifferent to the harm that results. Even if the
completed HNR is forwarded to health care staff, it is not processed
in a timely manner, so prisoners have to file multiple HNRs and face
long delays of many weeks and often months before they receive
medicine or are examined by qualified clinicians, and experience harm
and unnecessary pain and suffering as a result.
30.
Oftentimes, medical staff members respond to a HNR stating only that
the prisoner is on a waiting list to see a physician, dentist,
psychiatrist, or outside specialist, even in response to HNRs
alleging serious injuries that require immediate action. Plaintiffs
Hefner, Gamez, and Swartz have received responses telling them to “be
patient” to HNRs alleging serious pain or injuries. Plaintiff Licci
was told by the Perryville Facility Health Administrator (FHA) that
she was “hindering [her] own care” by filing grievances and HNRs
about not seeing an outside specialist about numerous suspicious
masses on her reproductive organs. Plaintiff Verduzco, who has a
history of self-harm and multiple suicide attempts, filed a HNR
reporting headaches, that she was experiencing auditory
hallucinations, and that she needed help with her psychotropic
medication, begging, “I’m scarde [sic]. Confused.” She received
a written response three days later, stating “You will be put on
the waiting list to be seen.” A prisoner who had a stent implanted
at an outside hospital in August 2011 after a heart attack was
ordered by the surgeon to see a cardiologist within a month. The
prisoner has filed multiple HNRs asking to be referred to a
cardiologist, but the most recent response he received to his HNR in
January 2012 was “Medical aware. Please be patient. Thanks.”
Another prisoner with major disabilities and multiple chronic medical
problems received a response to one HNR stating, “due to the fact
that the provider has to see a large amount of inmates, the number of
issues addressed per inmate will be limited to one main issue.” He
was told in a different response that he “must learn to accept and
live with [the] reality” of pain and discomfort. A staff member
told a prisoner who filed multiple HNRs over a two-month period for
untreated high blood pressure, seeing stars, and having problems
getting out of bed, that a two month wait for medical care is
acceptable, and that he should “pray” for his health issues to be
cured.
31.
Defendants have been warned repeatedly about these unreasonable
delays in access to health care. In April 2009, a physician at the
Eyman complex sent an email entitled “Deficient access to care,
Risk exposure” to Defendant Pratt’s predecessor as Health
Services Director, Dr. Adu-Tutu, and other prison officials, noting
it took prisoners “about 6 weeks to be seen” after the medical
department receives a HNR, and that the situation was a “multi car
accident waiting to happen.” The delays have only grown worse: in
February 2011 a Perryville psychiatrist warned Dr. Ben Shaw, the
Director of Mental Health Services who reports to Defendant Pratt,
that “we are backed up 3-4 months with the HNRs and longer for
regular follow-ups.”
32.
Lengthy delays in responding to HNRs and providing necessary health
care are the system-wide norm, as reflected in countless examples.
Plaintiff Hefner filed multiple HNRs in the spring of 2011 about pain
and injuries to his ribs and torso after an attack, but was not seen
by a doctor for three months. Plaintiff Polson has recurrent ear
infections, but when he has them he must file multiple HNRs and wait
anywhere from three to six weeks to be seen and given antibiotics or
ear drops.
33.
This failure to timely respond to HNRs is compounded by Defendants’
failure to create an effective tracking and scheduling system for
health care appointments or of prisoners’ medical records. There
also are no standardized protocols or timeframes dictating deadlines
by which a prisoner requesting care must receive a face-to-face
appointment with a nurse, doctor, or other clinician. As a result,
inadequately-trained lower-level staff triage the HNRs and decide
whether to schedule an examination, without sufficient information.
34.
The harm from the delays in care is aggravated by Defendants’
policy and practice of having ADC clinicians make treatment decisions
without examining prisoners, instead relying on brief notes or
descriptions from lower-level medical assistants and even
correctional officers who have no medical training. In the
unsupervised gatekeeping role Defendants force on them, these lower
level medical and custody staff often do not recognize or acknowledge
the symptoms a patient displays until the condition has become so
acute as to be life threatening or results in permanent injury. For
example, Plaintiff Polson had chronic ear infections for months that
were not being cured with basic antibiotics. During that time, he was
only seen by a Licensed Practical Nurse (LPN) or medical assistant
who would consult with a doctor over the phone; the physician would
not physically examine him. He had blood oozing out of his ear after
multiple ear infections, but was told by a physicians’ assistant
and a LPN that it was just a scratch. Due to Mr. Polson’s recurrent
untreatable infections and a prior diagnosis of the particularly
antibiotic-resistant methicillin-resistant staphylococcus aureus
(“MRSA”), the minimum standard of care requires the physician to
personally examine Mr. Polson and culture his ear to make sure a
different medicine would work. This was not done, and Mr. Polson
suffered permanent hearing loss.
35.
Plaintiff Hefner has a complicated ophthalmological history including
surgery for glaucoma and cataracts, and experiences iritis (recurrent
inflammation of the iris) after being given expired eye drops by a
prison nurse in 2006. He submitted seven HNRs for eye pain and
problems between August 2009 and October 2011. Because HNRs are not
reviewed by a physician or clinical staff member, the staff who
review the HNRs have repeatedly chosen to triage his request by
placing him on a waitlist to see an optometrist, rather than an
ophthalmologist. As of January 2012, he still had not yet seen an
ophthalmologist, despite twice being referred by the optometrist.
36.
Defendants also have a policy and practice of relying on unqualified
personnel to perform medical procedures for which they are
unqualified, with horrific results. For example, Plaintiff Jensen had
prostate cancer surgery in July 2010 and returned to the Tucson
prison with an internal Foley catheter connecting his bladder to his
urethra through the bladder neck. The catheter was to stay in place
for three weeks and be removed only by the outside urologist or
surgeon. Two weeks after his return, the catheter began to leak
urine. Mr. Jensen submitted two HNRs but was not seen until 48 hours
later by a nurse who said he could wait until his scheduled follow-up
appointment. The next day, still experiencing pain and leaking urine,
he was seen by a nursing assistant (“NA”) who requested a
doctor’s order to irrigate the Foley catheter. The physician did
not examine Mr. Jensen before authorizing the procedure. When the NA
attempted to irrigate Mr. Jensen’s catheter, she instead shoved it
deeper inside him and twisted it 180 degrees, causing excruciating
pain. The improper manipulation of the catheter tore out his internal
stitches, and the catheter ended up outside his bladder, lying freely
in his abdomen, such that urine drained from his torn bladder
directly into his abdominal cavity. Despite Mr. Jensen’s
excruciating pain, and the absence of urine, he was not taken to the
ER or to see an outside specialist until his previously scheduled
follow-up appointment three days later, at which point the outside
clinicians rushed him to the operating room for emergency surgery. As
a result of the injuries sustained during the NA’s attempt to
irrigate the catheter, he has required multiple follow up surgeries
to repair the bladder, remove scar tissue, and treat infections. In
February 2012, Mr. Jensen was told by an outside urologist that he
needed surgery to replace his irreparably destroyed bladder.
B.
Defendants Do Not Provide Prisoners With Timely Emergency Treatment
37.
Defendants Ryan and Pratt have a policy and practice of not providing
prisoners with timely emergency responses and treatment, and do not
have an adequate system for responding to health care emergencies.
38.
There is not an adequate number of on-duty health care staff to
respond to possible emergencies. For example, the Tucson complex’s
Whetstone Unit, designated for prisoners with the gravest and most
complex medical needs, does not have clinical staff on duty between
the hours of 6 pm and 6 am.
39.
Defendants have not adequately trained security and health care staff
on how to handle health care emergencies, and as a result of this
failure to respond properly and timely to emergencies, prisoners
suffer avoidable harm and injuries, including unnecessary deaths.
While trained in basic first aid, correctional officers are not
trained to evaluate medical situations. Yet correctional staff act as
gatekeepers, making critical decisions about whether emergency care
is warranted. In July 2010, correctional officers at the Tucson
prison stood by and watched a severely mentally ill prisoner named
Tony Lester bleed to death after his second suicide attempt. Mr.
Lester, who had paranoid schizophrenia, multiple personality
disorder, and auditory hallucinations, had been taken off suicide
watch, taken off his medications, and housed in the general
population, where he was given a hygiene kit that included a razor.
He used the razor blade to slit his throat, groin, and wrists, and he
wrote the word “VOICES” in his blood on an envelope. An ADC
internal investigation found that the four responding officers stood
by and did not administer any basic first aid. One officer told
investigators he didn’t want to be “wallowing through” Mr.
Lester’s blood, and another said his limited training did not teach
him how to stop bleeding. When an internal investigator asked one
officer, “So you guys just stood around for 23 minutes and watched
this guy bleed to death?”, the officer stated that his response was
to call Mr. Lester’s name and to try to elicit a reaction.
40.
In October 2011, a prisoner at the Eyman prison collapsed in his
living unit from a heart attack. Other prisoners yelled for security
staff to contact medical staff. Officers told the prisoners to “wait
and see what happens,” and did not summon help or provide
assistance to the stricken prisoner. In desperation, another inmate
checked the prisoner’s pulse, and finding none, began to perform
CPR. After a few minutes, the prisoner began breathing again. Only
then did officers summon medical staff. Three hours later, the
prisoner was sent from the medical unit back to his living unit and
told he had a medical appointment in a few days. The prisoner had
another heart attack the next day and died. After his death, the
prisoner who saved his life after the first heart attack by
performing CPR was issued a disciplinary write-up for violating a
rule that prisoners may not perform medical procedures on other
inmates.
41.
It is not only correctional staff that lack necessary training in
responding to emergency situations. Lower level medical staff, who
serve as the first line of response to prisoners’ requests for
medical assistance, often do not recognize when a prisoner is
experiencing an emergency. In September 2011, Plaintiff Swartz
swallowed a metal spring and copper wire, and told medical staff he
had done so. The mental health staff members did not believe him and
joked about how they would need to cut him open. They had him
screened with a metal detector or metal wand, and told him he would
have to wait to pass the pieces of metal. Using a metal detector to
detect the presence of objects in adults does not comport with the
appropriate standard of care, which requires physicians to obtain
X-rays and/or CT scans to determine the location of the object, and
to emergently remove sharp objects from the esophagus, stomach, or
small intestine via endoscopy. Mr. Swartz had an X-ray the following
day, after he swallowed yet another object, this time a sharpened
paper clip. The X-ray revealed multiple pieces of metal in his
stomach, including the spring and paper clip, but the prison doctor
did not refer him for an endoscopy, and instead told Mr. Swartz he
would have to pass the objects, which he did painfully several weeks
later. Ignoring sharp ingested objects puts a patient at risk for
perforation of internal organs and death.
42.
In another example, in May 2011, a prisoner who was four months
pregnant began experiencing painful contractions and spotting blood,
and went to Perryville’s medical unit. The staff person on duty
told her it was nothing serious, that her problems were “all in
your head,” and that she could not see a clinician for evaluation
or treatment. She was sent back to her living unit, and she continued
to experience great pain and cramping for an hour and a half, until
she miscarried.
43.
Even when properly responding to an emergency, medical staff face
barriers to providing timely emergency assistance. For example, a
prisoner in the Yuma prison has three to four seizures per week
because he does not regularly receive epilepsy medication. He
regularly encounters delays in the emergency response during his
seizures because of the configuration of his living unit – the
entrance door is 34 inches wide, and facing the entrance is a wall
approximately four feet high. As a result, medical staff cannot get a
gurney through the doorway without spending critical time contorting
the gurney through the door and around the wall. Other prisoners or
officers must help lift the gurney over the wall, or drag the
convulsing prisoner to the door of the unit.
C.
Defendants Fail to Provide Necessary Medication and Medical Devices
to Prisoners
44.
Defendants have a policy and practice of failing to prescribe,
provide, and properly manage medication, or of only providing
incorrect, interrupted, or incomplete dosages of medication.
Defendants also have a policy and practice of failing to provide
necessary medical devices and supplies. Prisoners experience delays
and gaps in receiving medicine or supplies, including those
prescribed by outside doctors. Delays and gaps also occur when
prisoners transfer from one ADC prison to another. Prisoners face
abrupt discontinuation of their medications for weeks or months,
before being seen by a new provider. For example, Plaintiff Swartz
was transferred in December 2011 from Phoenix to Lewis, but had to
file multiple HNRs and wait several weeks before he began receiving
the psychotropic medications prescribed by Phoenix physicians.
45.
Defendants have a policy and practice of not providing prisoners with
the full course of their medication, not providing prisoners
medication as prescribed or in a timely fashion, and inappropriately
starting and stopping medication. As a result, prisoners suffer
unnecessary harm, and in the cases of prisoners with psychotic and
mood disorders, suffer withdrawal symptoms and the recurrence of
symptoms such as hallucinations and suicidal ideation. For example,
Plaintiff Parsons’ medications were abruptly discontinued without
any clinical explanation and he was not seen for his resulting
psychiatric problems for two weeks. At that point he was prescribed
an entirely different medication.
46.
Psychotropic medications that are to be taken daily regularly go
undelivered, without explanation or warning. Plaintiff Gamez has had
medications abruptly started, stopped and restarted, including a
potent antipsychotic medication. Plaintiff Rodriguez was switched
multiple times from Risperdal to Haldol to treat her psychosis, but
with no documented explanation for the changes, and with a more rapid
titrating on and tapering off the medications than is consistent with
the therapeutic indications of use.
47.
Prisoners also are given expired medication or incorrect dosages of
medication, resulting in harm. When Plaintiff Hefner originally
suffered his eye injury, a nurse at the Safford prison gave him eye
medication that had expired more than three months previously. When
he used the medication, his vision dramatically worsened, and he
developed iritis. A prisoner at the Tucson complex was given the
incorrect dosage of medication to treat his seizures in September
2011. He suffered a stroke, and despite pleas for help from his
fellow inmates, waited more than a day before medical staff saw him
and referred him to an outside hospital’s Intensive Care Unit. Now,
due to the stroke, he slurs his speech, has difficulty walking and
relies on a wheelchair, and is incontinent.
48.
Defendants have a policy and practice of only providing medicine
listed on a limited formulary of approved medication, and routinely
substitute doctor-approved drug regimens with drugs on the
ADC-approved formulary. As a result of this policy and practice,
prisoners are deprived of medications that are well-established as
effective for their health conditions, and receive inferior,
ineffective, or obsolete medications, or nothing at all. For example,
when Plaintiff Brislan was incarcerated, mental health staff
discontinued his prior, effective medications because they were not
listed on the formulary. Instead, he was prescribed Buspar, an older
anti-anxiety medication, even though he told the nurse it had not
worked for him in the past. His mental health symptoms continued to
worsen while on Buspar. Plaintiff Parsons was given a potent
antipsychotic medication for hyperactivity, a condition for which the
drug is not normally prescribed, and had other psychiatric
medications discontinued several times. On multiple occasions,
Plaintiff Gamez was prescribed antipsychotic and anti-epileptic
medications such as Thorazine and Tegretol for off-label treatment of
irritability and mood disorder caused by a childhood traumatic brain
injury, even though there are other drugs that are more effective for
treating these symptoms, with fewer side effects.
49.
According to the 2011 deposition testimony of one of ADC’s doctors,
the prescription of non-formulary medication is frequently subject to
delay and erroneous denial. ADC policies restricting these
prescriptions result in multiple requests by prison doctors over
months until an ad-hoc committee of medical and administrative staff
at ADC’s central office reviews the request. As a result, prisoners
experience delays in treatment and unnecessary harm. For example,
Plaintiff Swartz went for more than six weeks without medication for
pain from his serious injuries and broken facial bones from an
assault, while awaiting central office approval of the physician’s
prescription for Tramadol. However, he was not prescribed a different
pain medication on the formulary list pending the approval of
Tramadol. Without the medication, he experienced intense pain and had
problems eating.
50.
Defendants have a policy and practice of not providing medically
necessary devices, thus depriving these prisoners of basic
sanitation. Plaintiff Jensen and other prisoners who need catheters
are given fewer clean catheters than they need, and thus have to
re-use the catheters, putting them at risk of bladder and urinary
tract infections. Plaintiff Jensen has repeatedly not been provided
an adequate number of catheters, and at times has had to rely on his
wife to order and pay for the catheters, and have them delivered to
the prison. Prisoners who need incontinence briefs or wipes often go
without them, or are told they only are allowed one diaper per day.
As with Plaintiff Jensen, prisoners fortunate enough to have the
assistance of family members often rely on them to obtain toileting
supplies and have them delivered to the prison.
D.
Defendants Employ Insufficient Health Care Staff
51.
Many of the severe deficiencies in ADC’s health care system are
caused by Defendants’ failure to employ sufficient health care
staff positions to provide adequate health care to prisoners. There
are simply insufficient medical, dental, and mental health clinicians
(i.e. physicians, psychiatrists, dentists, physicians’ assistants,
registered nurses, and other qualified clinicians) on staff to meet
the significant and documented health care needs of the almost 33,100
prisoners in ADC custody.
52.
As an ADC doctor at the Florence prison testified in September 2011,
“we are chronically and consistently understaffed.” The same
doctor had previously noted this problem in an email to prison staff,
stating that “[s]omething bad is going to happen sometime” and
pleading for help. In an email to Defendant Pratt’s predecessor,
Dr. Adu-Tutu, and other administrative and medical officials, this
same physician noted that “[w]e just don’t have the man power to
do our assigned duties,” are “unable to meet our policy and
constitutional mandates,” and the provision of health care
“continue[s] to be a multi-car accident waiting to happen.” And
in an email to other ADC medical staff, the doctor noted that
“inadequate staffing levels and unrealistic workloads lead to
significant breakdowns in the front line services we are trying to
provide” and concluded that “we are not meeting our own or
anybody else’s standard of care.”
53.
Defendants’ policy and practice of chronically and consistently
understaffing health care positions results in multiple deficiencies
and inadequate health care: there is not enough staff to timely
respond to prisoners’ requests for health care and to emergencies,
to provide uninterrupted medication delivery, or to adequately
screen, monitor and provide follow-up care to prisoners with serious
and chronic illnesses. The inadequate health care staffing is caused
by Defendants’ systematic elimination of health care staffing
positions in recent years, including physicians, dentists, registered
nurses, and psychiatrists, and Defendants’ failure to actively
recruit, hire, train, supervise and retain sufficient and competent
health care staff.
54.
Despite rising health care costs across the country, ADC spending on
health care staff positions dropped more than $4.4 million, or 8.4%,
from Fiscal Year (“FY”) 2009 to FY 2011 while the overall state
prison population declined by less than 1%. These positions were
eliminated despite warnings from Defendants’ own health care staff
that prisoners would suffer serious harm from the resulting delays in
access to care, emergency response, specialty care referrals, and
inadequate chronic care and medication management. For example, in
February 2011, the sole psychiatrist on staff at Perryville – a
complex with 3,500 prisoners and multiple special mental health units
for female prisoners – wrote an email entitled “Please help” to
prison officials, warning them that mental health staffing was
“abysmal,” and as a result mental health staff had to “renew
meds for dozens of people per week without getting to see them
because there is not enough time.” The psychiatrist concluded, “I’m
doing the best I can but it is still not enough. I do not want to
leave my position here as I feel that I do some good for the women
here and society in general but I am stretched very thin.” In June
2011 the same psychiatrist wrote an email entitled “Please assist
Florence” to Defendant Ryan and Defendant Pratt’s predecessor Dr.
Adu-Tutu, and other ADC officials describing the “dire situation”
at Florence as it was the last day that complex would have a
psychiatric provider. She described the problems the remaining
low-level staff were having in providing medication for prisoners.
Defendant Ryan’s response was, “Your concerns are not falling on
‘deaf ears’. I acknowledge your messages.”
55.
The harm resulting from staffing shortages is not limited to
Perryville and Florence. The Deputy Medical Director for Psychiatry
at Eyman warned Defendant Ryan and Dr. Adu-Tutu in a series of emails
in the fall of 2009 that prisoners “are not receiving a reasonable
level of psychiatric care. We are out of compliance with our own
policies regarding minimum frequency of contact with a provider, as
well as community standards for adequate care. The lack of treatment
represents an escalating danger to the community, the staff and the
inmates.” Defendant Ryan responded with a brusque one sentence
response that “a strategy is being pursued.”
56.
That strategy, if one was indeed pursued, has failed. As of August
2011, more than half of all mental health staff positions were vacant
at the Eyman complex, which houses multiple mental health units and
two SMUs, where prisoners are held in isolation. As of October 31,
2011, there was not a single psychiatrist on staff for the entire
Eyman complex. Nor are any psychiatrists currently employed on staff
at the Florence, Lewis, and Tucson complexes, which along with Eyman
are designated to house prisoners classified as “MH-4: High Need,”
signifying the prisoners need specialized placement in a mental
health program and intensive psychiatric staffing and services. As of
August 2011, the Yuma prison housed 52 prisoners classified as MH-3,
which ADC’s criteria describe as prisoners who require “regular,
full-time psychological and psychiatric staffing and services” and
who need mental health treatment and supervision. Yet as of November
2011, the only mental health staff person for the entire Yuma complex
was a lower-level, Psychology Associate II. That position does not
require medical training or a Ph.D., but rather only a degree in
counseling or social work. A Psychology Associate II cannot manage or
prescribe medications under current state law, and should be
supervised by a psychologist.
57.
Defendants have knowingly ignored the warnings of their own staff and
others about the staffing shortages, and as a result prisoners
continue to suffer from constitutionally inadequate health care and
substantial risk of serious harm due to
Defendants’
deliberate indifference to the impact of the system-wide staffing
shortages.
II.
Even If Prisoners See Health Care Providers, They Do Not Receive
Adequate Medical, Dental, or Mental Health Care
A.
Substandard Medical Care
58.
Plaintiffs Jensen, Swartz, Chisholm, Licci, Hefner, Polson, and
Wells, and the Medical Subclass, allege the following. Defendants
Ryan and Pratt have a policy and practice of failing to provide
prisoners with adequate medical care, and are deliberately
indifferent to the fact that the systemic failure to do so results in
significant injury and an substantial risk of serious harm to
prisoners. Defendants’ failure to provide adequate medical care
results in prisoners experiencing prolonged, unnecessary pain and
suffering, preventable injury, amputation, disfigurement, and death.
1.
Defendants Fail to Provide Prisoners With Care for Chronic Diseases
and Protection From Infectious Disease
59.
Defendants have a policy and practice of failing to provide prisoners
with medically necessary care to address ongoing medical needs or
diseases. Defendants’ deliberate indifference to their systemic
failure to properly treat or manage prisoners’ chronic illnesses
exacerbates prisoners’ conditions, and frequently leads to
preventable permanent injuries or deaths. For example, a prisoner who
needed medical care for gastrointestinal bleeding and an untreated
hernia tragically did not receive proper treatment even after
Defendants were aware of his problems. His hernia ruptured his
stomach lining and he was found dead after “vomiting up his
insides,” according to witnesses. Prior to his death, he reported
that a prison doctor told him the hernia was “merely cosmetic,”
yet when the prisoner asked about his prognosis, the doctor joked, “I
wouldn’t go to Vegas with you.” A prisoner who has Hepatitis C
requested treatment in a HNR, but was told in response that since he
had received a disciplinary ticket, he was not eligible for treatment
until one year after the date of the ticket.
60.
Defendants also have a policy and practice of not providing medical
diets ordered by clinicians for prisoners with chronic conditions
such as high blood pressure, high cholesterol, kidney failure, and
diabetes. Instead, all prisoners, including those with chronic
conditions requiring special diets, are given a nutritionally
inadequate, high-fat and high-sodium diet. Plaintiff Hefner has
chronic gastroesophageal reflux disease (GERD) and requires a special
diet. However, his request for a medical diet was denied, and the
meals he is given often aggravate his condition, forcing him to
choose between eating food that will cause physical distress, or
eating nothing.
61.
Defendants also have a policy and practice of failing to effectively
enforce state law prohibiting smoking inside buildings, endangering
the health of prisoners and Defendants’ employees with chronic
medical conditions such as asthma, chronic obstructive pulmonary
disease, allergies, or emphysema, and posing a health risk to
prisoners and staff exposed to second-hand smoke. Plaintiffs Gamez
and Thomas both have asthma, and report that second-hand cigarette
smoke has triggered asthma attacks.
62.
Defendants have a policy and practice of failing to mitigate the risk
of infectious and communicable diseases, such as MRSA,
Vancomycin-Resistant Enterococcus (VRE), Hepatitis C, and
tuberculosis. Defendants fail to maintain basic sanitation to prevent
the exacerbation of chronic conditions and the spread of infectious
diseases. Many sections of ADC’s prisons are filthy, fail to meet
basic sanitation standards, and expose prisoners to serious, and
sometimes fatal, communicable diseases. These conditions include
urine-soaked mattresses, uncontrolled infestations of vermin, and
cell walls and floors covered with black mold or smeared with the
feces, spit, and blood of other inmates. Prisoners with cuts or other
injuries to their bodies have contracted serious infections from the
unsanitary conditions of the prison. A prisoner living in unsanitary
conditions in the Tucson complex developed a staph infection but was
not examined by medical staff until the infection had spread to his
eyes. He now has minimal vision in his right eye and has lost vision
in his left eye.
2.
Defendants Fail to Provide Timely Access to Medically Necessary
Specialty Care
63.
Defendants have a policy and practice of failing to provide prisoners
with specialty care, or doing so only after extensive and
unreasonable delays, often resulting in unnecessary pain and
suffering, permanent injuries, and death. Defendants do not employ
medical specialists, but instead send prisoners to contracted outside
specialists. In 2009, reimbursement rates for prison medical
contractors were capped so as to be no higher than those paid by the
State’s Medicaid program, the Arizona Health Care Cost Containment
System. Defendants knew of the impending change to the reimbursement
system, but failed to take steps to ameliorate the foreseeable impact
of the change in policy. As a result, all outside medical providers
ended their contracts with ADC. For much of 2009 and 2010, Defendants
had no contracts in place with outside providers, and even today
have few outside specialists under contract to treat ADC prisoners.
Prior to the rate change, ADC’s spending on outside medical
services in FY 2009 was $70,860,190. In FY 2011, the first full year
following the change in rates, spending on specialty services had
plummeted by 38% to $43,807,120, while there was no corresponding
decline in the number of prisoners in ADC’s custody. Two years
later, as a result of the accumulation of pending referrals and the
smaller number of contracted providers, prisoners still encounter
lengthy delays in getting specialized care for serious medical needs.
64.
Defendants have been warned repeatedly by their own prison doctors
and are well aware that delays in referrals, including those caused
by an overly burdensome approval process for outside specialists harm
prisoners, but Defendants are deliberately indifferent to the
resulting harm. An ADC physician testified that it takes months for
specialty referrals to be processed and that physicians are not
notified of the decision from ADC headquarters as to whether the
referral will be granted. This doctor told prison officials “the
referral system has broken down.” Another ADC physician described
in an email to prison officials how difficult it was to refer to a
specialist a patient with a suspected carcinoma of the lip. After
repeatedly submitting urgent referrals, he finally sent the request
directly to the Division Director of Health Services. The physician
described a system where referrals are “falling through cracks,”
and estimated that “an extensive list of examples… would probably
exceed 30% of [his] consults.”
65.
Defendants’ policy and practice of systematically failing to
provide timely access to outside specialists causes prisoners
unnecessary harm. In late February 2010, Plaintiff Swartz was
attacked by other inmates and suffered eye injuries and fractures of
his cheek bone, orbital bone around his eye, and upper jaw bone –
fractures that, if not treated, result in the person’s face caving
in, and in permanent disfigurement. Outside emergency room doctors
advised that he be seen within a week by an ophthalmologist and
plastic surgeon. Prison doctors submitted these referrals to the
review committee, but they were not approved. Instead, Mr. Swartz was
sent to an oral surgeon, who operated on his face without an
anesthesiologist present. Mr. Swartz was over-sedated and had to have
an antidote to be revived. His face was partially paralyzed due to
nerve damage from the botched surgery and over-sedation, and his
eyelid drooped, causing dryness to his cornea. It was not until
almost eleven months after the injury that he finally saw an
ophthalmologist regarding his various injuries. Almost two years
after the attack, he has yet to have his eye and facial damage
repaired by a specialist.
66.
In another tragic case, medical staff at the Tucson prison complex
did not diagnose, treat, or refer to specialists a prisoner named
Ferdinand Dix who had untreated small cell lung cancer that had
spread to his liver, lymph nodes, and other major organs, causing
sepsis, liver failure, and kidney failure. For two years, Mr. Dix had
filed multiple HNRs and exhibited many symptoms consistent with lung
cancer, including a chronic cough and persistent shortness of breath,
and he tested positive for tuberculosis. Due to the metastasized
cancer, Mr. Dix’s liver was infested with tumors and grossly
enlarged to four times normal size, pressing on other internal organs
and impeding his ability to eat, but no medical staff even performed
a simple palpation of his abdomen. Instead, medical staff told him to
drink energy shakes. When Mr. Dix was finally taken to an outside
hospital in a non-responsive state in February 2011, his abdomen was
distended to the size of that of a full-term pregnant woman, as seen
in the photograph below. Mr. Dix died from the untreated cancer a few
days after ADC finally sent him to the hospital.
67.
Defendants have a policy and practice of failing to order or approve
outside diagnostic testing, including biopsies of suspicious tumors
and growths, and are deliberately indifferent to the resulting harm
to prisoners. For example, Plaintiff Jensen waited more than two
years to have a biopsy of the mass in his prostate, because contracts
with outside providers were cancelled. By the time he was finally
seen and treated, the cancer was much worse, resulting in more
invasive surgery and the need to permanently use a catheter.
Beginning in 2010 Plaintiff Licci observed multiple masses growing on
her breasts, mouth, and arms, and reported discomfort in her cervix.
The masses were observable in physical examinations. She began
experiencing frequent diarrhea, nausea, exhaustion, weight loss,
pain, and other alarming symptoms. Ms. Licci has a family history of
cancer and was treated for cancer in 2001. Starting in December 2010
she requested testing and a prison doctor ordered a referral to an
oncologist. However, Ms. Licci was not sent to an oncologist and did
not receive a CT scan until late September 2011. At that time the
masses were described as “lighting [the CT scan] up like a
Christmas tree,” and the specialist ordered biopsies and a
colonoscopy. Still, the Perryville gynecologist insisted that nothing
was wrong with her. She finally had an MRI in December 2011, but it
was not properly administered. Ms. Licci had to file additional HNRs
and grievances before receiving a second MRI, which confirmed
multiple masses on both ovaries. She still has not seen an oncologist
or had biopsies.
68.
A prison physician submitted a request that Plaintiff Hefner have a
CT scan to rule out a rib fracture and injury to his spleen in March
2011 after he was injured in an attack, but the request was never
reviewed or completed. Mr. Hefner experienced persistent pain and
submitted three different HNRs in April and May of 2011, but was not
seen by a doctor until June 29, 2011, at which time the CT scan was
again requested. He did not get a CT scan until late October, 2011,
suffering unnecessary pain in the interim.
69.
When outside physicians see prisoners, they often prescribe treatment
regimens and medication. However, when prisoners return to prison,
Defendants fail to monitor symptoms or provide follow-up treatment
ordered by outside hospital physicians in accordance with the
prescribed treatment regimens and medical standards of care. As a
result, prisoners suffer infections and unnecessary setbacks in their
recovery and must return to the hospital.
B.
Substandard Dental Care
70.
Plaintiffs Swartz, Parsons, Chisholm, Polson, and Wells, and the
Dental Subclass, allege the following. Defendants Ryan and Pratt have
a policy and practice of failing to provide medically necessary
dental services, and are deliberately indifferent to the fact that
the systemic failure to do so results in injury and a substantial
risk of serious harm to prisoners.
71.
Prisoners wait months or years for basic dental treatment and suffer
significant pain and other harm. Plaintiff Polson was put on the
“routine care” waiting list for dental treatment even though he
has multiple teeth that are visibly missing or broken. The prison
dentist designated him as qualified for partial dentures in April
2008, but they were not fitted until April 2011. He regularly does
not receive his soft food diet. He also filed a HNR after a dead
front tooth broke, asking to be seen by the dentist, and to receive a
soft diet, and inquiring about the status of receiving the dentures.
The only response on the HNR was “You are requesting ROUTINE care.
You are on ROUTINE care list.” He was not seen by the dentist until
five months later.
72.
The primary dental service provided by Defendants is tooth
extraction, even if a much less invasive procedure such as a filling
is medically appropriate and necessary. Prisoners regularly face the
horrible dilemma of saving a tooth and suffering pain, or ending the
pain and losing a tooth that otherwise could be saved. Plaintiff
Swartz is currently in this position. Some prisoners initially refuse
the extractions, but eventually acquiesce after suffering pain for a
long period of time, or their condition worsens until extraction is
the only treatment option available. After Plaintiff Wells reported
missing fillings in two of her teeth in December 2010, the prison
dentist recommended they be extracted. She refused, and the dentist
told her to file an HNR requesting replacement fillings. Ms. Wells
endured pain for several months before her fillings were replaced;
however, in the process an adjacent tooth was cracked, exposing a
nerve. She was told by the dentist to submit another HNR to get that
tooth repaired. Several months later, she still has not received
appropriate care and suffers pain.
73.
Prisoners who are fortunate enough to get fillings are not given
permanent fillings, but rather temporary fillings that are not
designed to last more than a few months at most. Plaintiff Parsons
filed an HNR in June 2008 regarding a cavity, but was not seen until
September of that year, at which time he was given a temporary
filling. He filed four HNRs in 2009 complaining that the temporary
filling had fallen out of his tooth. Each time, he was given another
temporary filling that would fall out weeks later, and he would have
to restart the process.
C.
Substandard Mental Health Care
74.
Plaintiffs Gamez, Swartz, Brislan, Rodriguez, Verduzco, Thomas,
Smith, Parsons, Chisholm, and Polson, Plaintiff Arizona Center for
Disability Law, and the Mental Health Subclass, allege the following.
Defendants Ryan and Pratt have a policy and practice of failing to
provide prisoners with adequate mental health care, and are
deliberately indifferent to the fact that the systemic failure to do
so results in injury and a substantial risk of serious harm to
prisoners.
1.
Defendants Deny Mentally Ill Prisoners Medically Necessary Mental
Health Treatment, Including the Proper Management and Administration
of Psychotropic Medication, Therapy, and Inpatient Treatment
75.
Defendants have a policy and practice of denying treatment or
providing inadequate treatment to prisoners with serious mental
health needs. Because of chronic understaffing, mentally ill
prisoners have insufficient interactions with psychiatrists; many
receive at most a five- or ten-minute interactions once or twice a
year in which they are asked only if their medications are working.
According to Defendants’ own records, some contacts with mental
health staff are as brief as two minutes. As a result, clinicians
cannot make informed decisions about care. For example, Plaintiff
Gamez did not see a psychiatrist from 2007 to 2011, despite
exhibiting worsening mental health and behaviors such as paranoia,
anxiety, panic, and psychosis. Instead, a nurse practitioner merely
prescribed a variety of psychotropic medications, including drugs not
indicated for his diagnosis and behavior. On two separate occasions
when Plaintiff Brislan was placed in suicide watch for weeks for
engaging in self-harming behavior and suffering severe side effects
from a variety of psychotropic medications, he did not see a
psychiatrist for stretches of five and seven months.
76.
Since they possess at most a glancing familiarity with their
patients, clinicians are unable to meaningfully evaluate crucial
decisions affecting safety and health, such as the clinical
appropriateness of indefinite confinement in SMUs and other units
that hold prisoners in long-term isolation with minimal opportunities
for human interaction. For example, Plaintiff Gamez experienced
hallucinations and deterioration in his mental health due to abrupt
interruptions in his medication, yet for two years he never saw a
psychiatrist while in Eyman’s SMU. Similarly, while in Eyman’s
SMU, Plaintiff Thomas did not see a psychiatrist for almost a year
even though he had been moved to the suicide watch unit multiple
times.
77.
This systemic failure of mental health treatment extends to the
management of psychotropic medication. Defendants have a policy and
practice of failing to monitor and provide follow-up treatment after
prescribing psychotropic medications. In addition, prisoners who are
on psychotropic medications that increase heat sensitivity are
exposed to levels of heat that pose potentially lethal risks.
Defendants are aware of the resulting problems and the risk of
serious harm to prisoners. In June 2011, the sole psychiatrist at
Perryville emailed Defendant Ryan and other prison officials about
the “dire situation” at the Florence prison, as it was the last
day a psychiatric provider would be on staff. As a result of the
staff shortage, she said she was contacted by nursing staff at the
Florence prison, asking her to prescribe or renew medications for
patients she had never examined, and who were housed at a prison 90
miles away from where she worked. The psychiatrist told Defendants
that
These
are patients I have never met or treated. The liability for treating
patients without evaluating and monitoring them is not one I am
willing to undertake. It is unreasonable for administration to expect
that its (very few) providers that it has left to carry the burden of
treating patients unseen. In the past, I have been willing to fill
meds for a day or two until the patient could be seen by the facility
psych provider, but I am not willing to prescribe meds for long
periods of time without seeing the inmate. …I hope for the sake of
the patients and the staff at Florence that you will drop everything
else you are doing and work on getting a provider for them.
78.
Defendant Ryan’s response was “[y]our concerns are not falling on
‘deaf ears’.” Yet the problem the psychiatrist raised in June
continues. According to ADC staffing reports, as of November 2011,
four of the six prisons designated by Defendants for Level MH-4
seriously mentally ill prisoners – Eyman, Florence, Lewis, and
Tucson – do not have a single psychiatrist on staff; it is
therefore unclear who is writing or renewing prescriptions for
psychotropic medication at those complexes. The Phoenix facility,
which is located on the grounds of the Arizona State Hospital and is
designated for the highest two levels of prisoners in need of
inpatient mental health care, has only one psychiatrist on staff. As
of February 28, 2012, 197 prisoners were housed in these mental
health units at Phoenix.
79.
Because prisoners on psychotropic medications rarely if ever see a
psychiatrist due to staffing shortages, there is little or no
follow-up to evaluate the efficacy of prescribed medications, to
ensure that dosages are adjusted properly to achieve therapeutic
levels, or to evaluate prisoners for possible adverse side effects.
For example, Plaintiffs Parsons, Polson, and Gamez did not have their
blood regularly drawn to test for dangerous side effects of
medication. Similarly, without any documentation of the basis for
their decisions, mental health staff prescribed Plaintiff Rodriguez
high doses of Haldol, an old medication that carries a much greater
risk than newer medications of side effects and long QTc syndrome,
which puts a person at risk of heart arrhythmias. Ms. Rodriguez had a
history of long QTc measurements, and exhibited symptoms including
lack of spontaneous speech, muscle and jaw stiffness, involuntary
movements, and grimacing. Ms. Rodriguez finally started to refuse
Haldol because of the side effects, aggravating her symptoms of
mental illness. While housed in Eyman and Lewis prisons, Plaintiff
Brislan demonstrated ongoing self-harming behaviors and dangerous
side effects from multiple psychotropic medications, but he was
rarely evaluated by a psychiatrist to see if medication adjustments
might be helpful for his symptoms. Psychiatrists renewed the
prescriptions, but the clinical notes did not indicate that the
psychiatrist had ever seen Brislan, a clear violation of the
applicable standard of care.
80.
Defendants have a policy and practice of allowing ongoing monitoring
of prisoners on psychotropic medication by LPNs, psychology
assistants, or medication assistants who hand out the medications.
These lower level mental health staff are not qualified to adequately
convey a prisoner’s concerns to a psychiatrist. Furthermore, staff
at this level should not be ordering or authorizing the dispensation
of medication. Plaintiff Swartz saw only lower level mental health
staff at his cell front and did not see a psychiatrist for over a
year, even though he had multiple suicide attempts and was put on a
variety of psychotropic medication, and the dosages were regularly
changed. Similarly, in June 2008, Plaintiff Smith was prescribed
Celexa, but did not receive it for nearly a year. He was also
prescribed lithium; however, despite the need for close monitoring
for side effects from the lithium, he was not seen by a doctor for
three months. His lithium was renewed without Mr. Smith having seen a
doctor for six months. In November 2009, Mr. Smith submitted a HNR
reporting that he was vomiting when given lithium without food. He
was given Tums and was not seen by a doctor. When he reported
continuing symptoms in January 2010, he was told to submit another
HNR and was not seen by a doctor until March 2010, four months after
first reporting symptoms. Plaintiff Verduzco goes months without
seeing the Perryville psychiatrist, despite demonstrating multiple
symptoms of severe psychological distress including hallucinations
and acts of self-harm.
81.
According to Defendants’ own records, approximately 1,350 ADC
prisoners are “severely mentally ill.” Some of these prisoners
suffer from psychosis, a disorder that is marked by loss of contact
with reality and disorganized thinking. Persons suffering from
psychosis may have perceptual disturbances such as hallucinations,
paranoia, delusional beliefs, and bizarre behaviors. Some of these
very mentally ill prisoners require an inpatient level of care – a
structured program of psychosocial rehabilitation services coupled
with individual therapy and appropriate medication management – but
they do not receive it. Defendants have failed to reliably provide
inpatient mental health care to those prisoners whose serious mental
health needs require it. Plaintiffs Brislan, Rodriguez, and Verduzco
are among those who require but have not received inpatient mental
health care.
2.
Defendants Deprive Suicidal and Self-Harming Prisoners of Basic
Mental Health Care
82.
Defendants have a policy and practice of housing prisoners with
serious mental health needs in unsafe conditions that heighten their
risk of suicide. In FY 2011, there were 13 suicides in ADC prisons,
out of a population that averaged 34,000 during that time. That is a
rate of 38 suicides per 100,000 prisoners per year, more than double
the national average suicide rate in state prisons of 16.67 per
100,000. Three prisoners committed suicide in one week in late
January 2012, including a 19-year-old woman.
83.
One factor responsible for such a high suicide rate is Defendants’
policy and practice of maintaining suicide watch facilities that
offer no meaningful treatment. Usually the only people who interact
with prisoners on suicide watch are correctional officers who check
on them periodically, medication assistants who dispense pills, or
psychology assistants who talk to them through the front of their
cell. Plaintiff Swartz did not receive psychotherapy for more than
two months in the summer of 2011 while on suicide watch at the Lewis
facility. After he swallowed glass and was taken to an outside
hospital, the hospital psychiatrist recommended that he be taken to
an inpatient mental health unit. These units are in the Phoenix
complex. Instead, Mr. Swartz remained at Lewis where he continued to
harm himself. He finally was moved to the Phoenix inpatient unit
almost three months after the hospital psychiatrist had made that
recommendation, but after a short period of time he was again
returned to Lewis. Plaintiff Thomas did not see a psychiatrist for 11
months despite being placed on suicide watch multiple times.
84.
Defendants also have a policy and practice of holding suicidal and
mentally ill prisoners in conditions that violate all notions of
minimally adequate mental health care and basic human dignity, and
are not compatible with civilized standards of humanity and decency.
Suicide watch cells are often filthy, with walls and food slots
smeared with other prisoners’ blood and feces, reeking of human
waste. Mental health staff show a lack of professionalism and little
compassion for prisoners enduring these conditions: for example,
prisoners in suicide cells are taunted for being in “the feces
cells.” When Plaintiff Swartz complained to a LPN about the
unhygienic conditions of the suicide cell at Lewis, the LPN described
him in the mental health notes from the encounter as “bitching
about cleanliness – germs and disease.”
85.
Defendants have a policy and practice of keeping suicide watch cells
at very cold temperatures. Prisoners are stripped of all clothing and
given only a stiff suicide smock and a thin blanket, making the
extreme cold even harder to tolerate. Plaintiffs Rodriguez and
Verduzco report that the suicide smock used in Perryville barely
comes to the top of female prisoners’ thighs, so both their legs
and arms are exposed to cold air. Many prisoners are also deprived of
mattresses and as a result must sleep on bare steel bed frames, or on
the floor made filthy with the bodily fluids of prior inhabitants.
Plaintiff Brislan spent several weeks in a frigid suicide cell with
no mattress.
86.
Defendants have a policy and practice of exposing prisoners on
suicide watch to gratuitously harsh, degrading, and damaging
conditions of confinement. Prisoners are given only two cold meals a
day, and are denied the opportunity to go outside, brush their teeth,
or take showers. The only monitoring prisoners receive in suicide
watch is when correctional officers force them awake every ten to 30
minutes, around the clock, ostensibly to check on their safety. In
some suicide cells, bright lights are left on 24 hours a day. The
resulting inability to sleep aggravates the prisoners’
psychological distress.
87.
Mentally ill prisoners on suicide watch complain of correctional
staff behavior that interferes with any therapeutic effect of being
on suicide watch, including harassment, insults and taunts, and the
excessive and practically sporting use of pepper spray. Prisoners at
the Perryville suicide watch units, including Plaintiff Verduzco,
have jerked awake when awoken by staff on the “safety checks,”
and are pepper sprayed for allegedly attempting to assault the
officers. Guards in the Perryville suicide watch units also
frequently pepper spray female prisoners in their eyes and throats
when they are delusional or hallucinating. Plaintiffs Rodriguez and
Verduzco have asthma and rely upon inhalers, and they have had asthma
attacks from the regular use of pepper spray in the women’s suicide
watch unit. On multiple occasions after she was pepper sprayed in the
eyes, nose, and mouth, Ms. Verduzco was dragged to a shower, stripped
naked, and sprayed with extremely cold water to rinse away the pepper
spray; she was then left naked to wait for a new vest and blanket. A
prisoner in the Florence prison’s suicide watch unit reports that
while there he was handed razor blades to swallow by other prisoners,
and told “just die right away.” He started to swallow the blades,
and security staff pepper sprayed him while he coughed up blood, and
did not provide other emergency response.
88.
Defendants’ policy and practice of holding suicidal prisoners in
excessively harsh conditions does not prevent but rather promotes
self-injurious behavior. Plaintiff Brislan has cut himself numerous
times with razors and pieces of metal while on suicide watch at
multiple prisons, including Tucson, Lewis, and Eyman’s SMU 1 and
Browning units. At the Tucson prison, staff put him on suicide watch
in a cell with broken glass on the floor which he used to cut
himself. During another stay in suicide watch, Mr. Brislan was given
a razor blade that he used to deeply lacerate both of his thighs.
While on suicide watch in the Lewis prison during the summer of 2011,
Plaintiff Swartz, on separate occasions, swallowed multiple foreign
objects, including two large staples, plastic wrap, a piece of glass,
a lead-head concrete nail, a spork, two pens, sharpened paper clips,
a metal spring, a steel bolt, and two copper wires. As with Plaintiff
Brislan, Mr. Swartz’s repeated suicidal gestures and ability to
access dangerous objects while on suicide watch confirms that he was
not being properly monitored and that any mental health treatment he
might have been receiving was inadequate.
89.
Defendants also have a policy and practice of improperly using the
suicide watch cells to punish prisoners for alleged disciplinary
infractions. An Eyman prisoner who went on a hunger strike to protest
prison policies, but did not display signs of mental illness or
distress, was put in a suicide watch cell for several weeks and was
told by a mental health provider, “If you weren’t on this hunger
strike, you wouldn’t have to live in the feces cell.”
III.
Defendants Subject Prisoners in Isolation to Unconstitutional
Conditions
90.
Plaintiffs Gamez, Swartz, Brislan, Rodriguez, Verduzco, Thomas,
Smith, and Polson, Plaintiff Arizona Center for Disability Law, and
the Isolation Subclass allege the following. Defendants have a policy
and practice of confining thousands of prisoners in isolation
(defined as confinement in a cell for 22 hours or more each day or
confinement in Eyman – SMU 1, Eyman – Browning Unit, Florence –
Central Unit, or Perryville – Lumley Unit Special Management Area
(SMA)), in conditions of enforced idleness, social isolation, and
sensory deprivation, and are deliberately indifferent to the
resulting substantial risk of serious physical and psychiatric harm.
91.
The large majority of prisoners in isolation are held in four
facilities: two SMUs at the Eyman prison (SMU 1 and Browning Units);
the Florence complex’s Central Unit; and the Perryville complex’s
Lumley SMA for female prisoners. However, other prisoners are held in
isolation in Complex Detention Units (CDUs) and other restricted
housing units throughout ADC.
92.
Prisoners in isolation leave their cells no more than three times a
week, for a brief shower and no more than two hours of “exercise”
in the “rec pen” – a barren, windowless concrete cell with high
walls that is not much larger than the cells in which prisoners live,
with no exercise equipment. Many prisoners refuse to go to the rec
pen, because it is so small that it does not allow meaningful
exercise, and because prisoners are placed in restraints and
strip-searched when going to and returning from the rec pen. In
addition, prisoners sometimes are not allowed to take water to the
rec pen, even at the height of Arizona’s summer heat. For those
prisoners who do wish to go to the rec pen, even this brief respite
is often denied: exercise is sometimes cancelled due to staffing
shortages. Prisoners in Florence’s Central Unit, including
Plaintiff Gamez, are not allowed to go to recreation if they are not
clean-shaven, but are often deprived of shaving supplies and are thus
denied exercise. Some prisoners in isolation receive no outdoor
exercise at all for months or years on end; others receive
insufficient exercise to preserve their physical and mental health.
93.
Conditions of isolation are designed to minimize human contact and
environmental stimulation. Most or all of these prisoners are held in
cells with a solid steel door and no window to the outside. Some
prisoners have no means of telling the time and become disoriented
and confused, not knowing the date or whether it is day or night. The
cells are often illuminated 24 hours a day, making sleep difficult
and further contributing to prisoners’ disorientation and mental
deterioration. Chronic sleep deprivation is common. Plaintiff Thomas
reported an inability to sleep and requested Ambien, but was not
prescribed a sleep aid. Property is extremely limited. Many prisoners
have no radio or television, and many are illiterate or have
difficulty reading, leaving them in a state of enforced idleness with
nothing to do but sleep, sit, or pace in their cells.
94.
Prisoners in isolation often go months or years without any
meaningful human interaction. Unless they are fortunate enough to
receive a brief medical or legal appointment or a visit, prisoners
are isolated from virtually all human contact. Their only regular
interaction with another human being occurs when officers deliver
their food trays, or place them in restraints and strip-search them
while taking them to or from the rec pen.
95.
Defendants have a policy and practice of denying prisoners in
isolation adequate nutrition, which Defendants justify on the basis
that, because these prisoners receive virtually no exercise, they
burn fewer calories and therefore need less food. Some prisoners in
isolation receive only two meals per day, which do not meet their
minimal nutritional needs. Prisoners experience constant hunger pangs
and some lose significant weight as a result of Defendants’ policy
of providing inadequate nutrition. Plaintiff Thomas lost 30 pounds
while in isolation. Plaintiff Smith, who is in isolation supposedly
for his own protection after leaving a gang, often cannot eat the
limited amount of food he is given, as it is tampered with by the
prisoner kitchen workers who target him for retaliation. He has
complained to prison staff, to no avail.
96.
The devastating effects of these conditions of extreme social
isolation and environmental deprivation are well known to Defendants.
An abundant psychiatric literature spanning nearly two hundred years
has documented the adverse mental health effects of isolation, and
Arizona prisoners are no exception. Even prisoners who have no mental
illness when first placed in isolation often experience a dramatic
deterioration in their mental health, developing symptoms such as
paranoia, anxiety, depression, and post-traumatic stress disorder.
For example, Mr. Thomas did not suffer from suicidal ideation when he
was put in isolation, but as time went on, his mental and physical
state deteriorated. He developed suicidal ideation and physically
harmed himself several times. Plaintiff Smith’s file notes that on
January 5, 2010, he reported mental health problems while housed in
isolation, but he could not be seen due to a “psych RN shortage.”
Even those prisoners who withstand isolation better than most are
subjected to intolerable conditions, as they are forced to endure the
hallucinations and screaming of prisoners suffering the debilitating
effects of isolation.
97.
Isolation is even more predictably damaging to prisoners with a
pre-existing mental illness. For these prisoners, isolation poses a
grave risk of exacerbation of mental health symptoms, psychiatric
injury such as PTSD, self-harm, and suicide. Deprived of the social
interaction that is essential to keep them grounded in reality, many
prisoners with mental illness experience catastrophic and often
irreversible psychiatric deterioration. Unlike prison officials in
many states, Defendants’ policy and practice allows the isolation
of prisoners with mental illness, and Defendants knowingly hold
prisoners designated as seriously mentally ill in isolation.
98.
The harm to prisoners in isolation is exacerbated by the policy and
practice of Defendants of failing to provide adequate mental health
care staffing and treatment. In addition, the harsh regime and severe
limits on human contact in isolation render appropriate mental health
treatment effectively impossible. Prisoners in isolation do not
receive regular contact with psychiatrists or mental health
clinicians, nor do they receive the limited group therapy that is
sometimes provided to prisoners in other ADC facilities. Defendants
stated in response to a public records request that they keep no
records of the mental health programming provided to prisoners in
isolation. These prisoners’ rare interactions with mental health
staff usually consist of “cellfront” contacts in which the staff
member shouts through the cell door, within earshot of both officers
and other prisoners. There is currently no psychiatrist on staff at
Eyman, which has two SMUs.
99.
The most common form of mental health treatment for prisoners in
isolation is the administration of powerful psychotropic medications,
with little or no supervision by a psychiatrist. For example,
Plaintiff Gamez was not seen by a psychiatrist from 2007 through 2011
despite worsening mental health symptoms. His mental health
deteriorated extensively while held in isolation from 2009 through
2011, yet he did not see a psychiatrist or receive psychotherapy
despite filing multiple HNRs detailing his symptoms. Similarly,
Plaintiffs Brislan and Swartz had psychotropic medications renewed
without any contact with a psychiatrist, despite increasing incidents
of self-harming behavior and side effects while in isolation.
Prisoners who require an inpatient level of mental health care, like
Plaintiffs Brislan and Verduzco, do not receive it, and are instead
left in isolation where their condition worsens.
100.
The predictable outcomes of these cruel conditions of isolation are
psychiatric deterioration, self-injury, and death. Plaintiffs Swartz
and Brislan attempted to commit suicide on multiple occasions while
in isolation. Recently a prisoner with depression who was housed in
isolation at Florence-Central Unit repeatedly asked custodial staff
and medical staff passing by if he could be seen by mental health
because he was suicidal. Nothing was done for him, and he committed
suicide by hanging on January 28, 2012.
CLASS
ACTION ALLEGATIONS
Plaintiff
Class
101.
All prisoner Plaintiffs bring this action on their own behalf and,
pursuant to Rules 23(a), 23(b)(1), and 23(b)(2) of the Federal Rules
of Civil Procedure, on behalf of a class of all prisoners who are
now, or will in the future be, subjected to the medical, mental
health, and dental care (collectively “health care”) policies and
practices of the ADC (the “Plaintiff Class”).
Numerosity:
Fed. R. Civ. P. 23(a)(1)
102.
The class is so numerous that joinder of all members is
impracticable. Fed. R. Civ. P. 23(a)(1). As of March 1, 2012, there
are approximately 33,100 prisoners in the custody of ADC’s prisons,
all of whom are dependent entirely on Defendants for the provision of
health care. Due to Defendants’ policies and practices, all ADC
prisoners, numbering tens of thousands annually, receive or are at
risk of receiving inadequate health care while in ADC prisons.3
103.
The Plaintiff Class members are identifiable using records maintained
in the ordinary course of business by the ADC.
Commonality:
Fed. R. Civ. P. 23(a)(2)
104.
There are questions of law and fact common to the members of the
class. Such questions include, but are not limited to:
(a)
whether Defendants’ failure to operate a health care system
providing minimally adequate health care violates the Cruel and
Unusual Punishments Clause of the Eighth Amendment,
(b)
whether Defendants have been deliberately indifferent to the serious
health care needs of class members.
Defendants
are expected to raise common defenses to these claims, including
denying that their actions violated the law.
3
This proposed class does not include the approximately 6,400 Arizona
prisoners housed in private for-profit prisons pursuant to contracts
with ADC.
Typicality:
Fed. R. Civ. P. 23(a)(3)
105.
The claims of the Plaintiffs are typical of those of the Plaintiff
Class, as their claims arise from the same policies, practices, or
courses of conduct; and their claims are based on the same theory of
law as the class’s claims.
///
Adequacy:
Fed. R. Civ. P. 23(a)(4)
106.
Plaintiffs are capable of fairly and adequately protecting the
interests of the Plaintiff class because Plaintiffs do not have any
interests antagonistic to the class. Plaintiffs, as well as the
Plaintiff class members, seek to enjoin the unlawful acts and
omissions of Defendants. Finally, Plaintiffs are represented by
counsel experienced in civil rights litigation, prisoners’ rights
litigation, and complex class action litigation.
Fed.
R. Civ. P. 23(b)(1)(A) and (B)
107.
This action is maintainable as a class action pursuant to Fed. R.
Civ. P. 23(b)(1) because the number of class members is approximately
33,100, and the prosecution of separate actions by individuals would
create a risk of inconsistent and varying adjudications, which in
turn would establish incompatible standards of conduct for Defendants
Ryan and Pratt. Additionally, the prosecution of separate actions by
individual members could result in adjudications with respect to
individual members that, as a practical matter, would substantially
impair the ability of other members to protect their interests.
Fed.
R. Civ. P. 23(b)(2)
108.
This action is also maintainable as a class action pursuant to Fed.
R. Civ. P. 23(b)(2) because Defendants’ policies, practices,
actions, and omissions that form the basis of this complaint are
common to and apply generally to all members of the class, and the
injunctive and declaratory relief sought is appropriate and will
apply to all members of the class. All state-wide health care
policies are centrally promulgated, disseminated, and enforced from
the central headquarters of ADC by Defendants Ryan and Pratt. The
injunctive and declaratory relief sought is appropriate and will
apply to all members of the Plaintiff class.
Medical
Subclass
109.
Plaintiffs Jensen, Swartz, Chisholm, Licci, Hefner, Polson, and Wells
bring this action on their own behalf and, pursuant to Rules 23(a),
23(b)(1), and 23(b)(2) of the Federal Rules of Civil Procedure, on
behalf of a subclass of all prisoners (hereinafter “Medical
Subclass”) who are now, or will in the future be, subjected to the
medical care policies and practices of the ADC. “Medical care”
includes care related to hearing and vision.
Numerosity:
Fed. R. Civ. P. 23(a)(1)
110.
The Medical Subclass is so numerous that joinder of all members is
impracticable. As of March 1, 2012, there are approximately 33,100
prisoners in the custody of ADC’s prisons, all of whom are
dependent entirely on Defendants for the provision of medical care.
Due to Defendants’ policies and practices, all ADC prisoners,
numbering tens of thousands annually, receive or are at risk of
receiving inadequate medical care while in ADC prisons.
111.
The Medical Subclass members are identifiable using records
maintained in the ordinary course of business by the ADC.
Commonality:
Fed. R. Civ. P. 23(a)(2)
112.
There are questions of law and fact common to the members of the
Medical Subclass. Such questions include, but are not limited to:
(a)
whether Defendants’ failure to operate a medical care system
providing minimally adequate medical care violates the Cruel and
Unusual Punishments Clause of the Eighth Amendment,
(b)
whether Defendants have been deliberately indifferent to the
resulting harm and risk of harm to Medical Subclass members who are
deprived of minimally adequate medical care.
Defendants
are expected to raise common defenses to these claims, including
denying that their actions violated the law.
Typicality:
Fed. R. Civ. P. 23(a)(3)
113.
The claims of the Plaintiffs are typical of those of the Medical
Subclass, because their claims arise from the same policies,
practices, or courses of conduct; and their claims are based on the
same theory of law as the subclass’s claims.
Adequacy:
Fed. R. Civ. P. 23(a)(4)
114.
Plaintiffs are capable of fairly and adequately protecting the
interests of the Medical Subclass because Plaintiffs do not have any
interests antagonistic to the subclass. Plaintiffs, as well as the
Medical Subclass members, seek to enjoin the unlawful acts and
omissions of Defendants. The Plaintiffs are represented by counsel
experienced in civil rights litigation, prisoners’ rights
litigation, and complex class action litigation.
Fed.
R. Civ. P. 23(b)(1)(A) and (B)
115.
Since the number of Medical Subclass members is so large, the
prosecution of separate actions by individuals would create a risk of
inconsistent and varying adjudications, which in turn would establish
incompatible standards of conduct for Defendants Ryan and Pratt.
116.
Additionally, the prosecution of separate actions by individual
members could result in adjudications with respect to individual
members that, as a practical matter, would substantially impair the
ability of other members to protect their interests.
Fed.
R. Civ. P. 23(b)(2)
117.
Defendants’ policies, practices, actions, and omissions that form
the basis of the claims of the Medical Subclass are common to and
apply generally to all members of the subclass, and the injunctive
and declaratory relief sought is appropriate and will apply to all
members of the subclass. All state-wide medical policies are
centrally promulgated, disseminated, and enforced from the central
headquarters of ADC by Defendants Ryan and Pratt. The injunctive and
declaratory relief sought is appropriate and will apply to all
members of the subclass.
Dental
Subclass
118.
Plaintiffs Swartz, Parsons, Chisholm, Polson, and Wells bring this
action on their own behalf and, pursuant to Rules 23(a), 23(b)(1),
and 23(b)(2) of the Federal Rules of Civil Procedure, on behalf of a
subclass of all prisoners (hereinafter “Dental Subclass”) who are
now, or will in the future be, subjected to the dental care policies
and practices of the ADC.
Numerosity:
Fed. R. Civ. P. 23(a)(1)
119.
The Dental Subclass is so numerous that joinder of all members is
impracticable. As of March 1, 2012, there are approximately 33,100
prisoners in the custody of ADC’s prisons, all of whom are
dependent entirely on Defendants for the provision of dental care.
Due to Defendants’ policies and practices, all ADC prisoners,
numbering tens of thousands annually, receive or are at risk of
receiving inadequate dental care while in ADC prisons.
120.
The Dental Subclass members are identifiable using records maintained
in the ordinary course of business by the ADC.
Commonality:
Fed. R. Civ. P. 23(a)(2)
121.
There are questions of law and fact common to the members of the
Dental Subclass. Such questions include, but are not limited to:
(a)
whether Defendants’ failure to operate a dental care system
providing minimally adequate dental care violates the Cruel and
Unusual Punishments Clause of the Eighth Amendment,
(b)
whether Defendants have been deliberately indifferent to the
resulting harm and risk of harm to Dental Subclass members who are
deprived of minimally adequate dental care.
Defendants
are expected to raise common defenses to these claims, including
denying that their actions violated the law.
Typicality:
Fed. R. Civ. P. 23(a)(3)
122.
The claims of the Plaintiffs are typical of those of the Dental
Subclass, because their claims arise from the same policies,
practices, or courses of conduct; and their claims are based on the
same theory of law as the subclass’s claims.
Adequacy:
Fed. R. Civ. P. 23(a)(4)
123.
Plaintiffs are capable of fairly and adequately protecting the
interests of the Dental Subclass because Plaintiffs do not have any
interests antagonistic to the subclass. Plaintiffs, as well as the
Dental Subclass members, seek to enjoin the unlawful acts and
omissions of Defendants. Finally, Plaintiffs are represented by
counsel experienced in civil rights litigation, prisoners’ rights
litigation, and complex class action litigation.
Fed.
R. Civ. P. 23(b)(1)(A) and (B)
124.
Since the number of Dental Subclass members is so large, the
prosecution of separate actions by individuals would create a risk of
inconsistent and varying adjudications, which in turn would establish
incompatible standards of conduct for Defendants Ryan and Pratt.
Additionally, the prosecution of separate actions by individual
members could result in adjudications with respect to individual
members that, as a practical matter, would substantially impair the
ability of other members to protect their interests.
Fed.
R. Civ. P. 23(b)(2)
125.
Defendants’ policies, practices, actions, and omissions that form
the basis of the claims of the Dental Subclass are common to and
apply generally to all members of the subclass, and the injunctive
and declaratory relief sought is appropriate and will apply
to
all members of the subclass. All state-wide dental policies are
centrally promulgated, disseminated, and enforced from the central
headquarters of ADC by Defendants Ryan and Pratt. The injunctive and
declaratory relief sought is appropriate and will apply to all
members of the subclass.
///
Mental
Health Subclass
126.
Plaintiffs Gamez, Swartz, Brislan, Rodriguez, Verduzco, Smith,
Parsons, Chisholm, and Polson, bring this action on their own behalf
and, pursuant to Rules 23(a), 23(b)(1), and 23(b)(2) of the Federal
Rules of Civil Procedure, on behalf of a subclass of all prisoners
(hereinafter “Mental Health Subclass”) who are now, or will in
the future be, subjected to the mental health care policies and
practices of the ADC.
Numerosity:
Fed. R. Civ. P. 23(a)(1)
127.
The Mental Health Subclass is so numerous that joinder of all members
is impracticable. As of March 1, 2012, there are approximately 33,100
prisoners in the custody of ADC’s prisons, all of whom are
dependent entirely on Defendants for the provision of mental health
care. Due to Defendants’ policies and practices, all ADC prisoners,
numbering tens of thousands annually, receive or are at risk of
receiving inadequate mental health care while in ADC prisons. The
Mental Health Subclass members are identifiable using records
maintained in the ordinary course of business by the ADC.
Commonality:
Fed. R. Civ. P. 23(a)(2)
128.
There are questions of law and fact common to the members of the
Mental Health Subclass. Such questions include, but are not limited
to:
(a)
whether Defendants’ failure to operate a mental health care system
providing minimally adequate mental health care violates the Cruel
and Unusual Punishments Clause of the Eighth Amendment,
(b)
whether Defendants have been deliberately indifferent to the
resulting harm and risk of harm to Mental Health Subclass members who
are deprived of minimally adequate mental health care.
Defendants
are expected to raise common defenses to these claims, including
denying that their actions violated the law.
Typicality:
Fed. R. Civ. P. 23(a)(3)
129.
The claims of the Plaintiffs are typical of those of the Mental
Health Subclass, because their claims arise from the same policies,
practices, or courses of conduct; and their claims are based on the
same theory of law as the subclass’s claims.
Adequacy:
Fed. R. Civ. P. 23(a)(4)
130.
Plaintiffs are capable of fairly and adequately protecting the
interests of the Mental Health Subclass because Plaintiffs do not
have any interests antagonistic to the subclass. Plaintiffs, as well
as the Mental Health Subclass members, seek to enjoin the unlawful
acts and omissions of Defendants. Finally, Plaintiffs are represented
by counsel experienced in civil rights litigation, prisoners’
rights litigation, and complex class action litigation.
Fed.
R. Civ. P. 23(b)(1)(A) and (B)
131.
Since the number of Mental Health Subclass members is so large, the
prosecution
of separate actions by individuals would create a risk of
inconsistent and varying adjudications, which in turn would establish
incompatible standards of conduct for Defendants Ryan and Pratt.
Additionally, the prosecution of separate actions by individual
members could result in adjudications with respect to individual
members that, as a practical matter, would substantially impair the
ability of other members to protect their interests.
Fed.
R. Civ. P. 23(b)(2)
132.
Defendants’ policies, practices, actions, and omissions that form
the basis of the claims of the Mental Health Subclass are common to
and apply generally to all members of the subclass, and the
injunctive and declaratory relief sought is appropriate and will
apply to all members of the subclass. All state-wide mental health
policies are centrally promulgated, disseminated, and enforced from
the central headquarters of ADC by Defendants Ryan and Pratt. The
injunctive and declaratory relief sought is appropriate and will
apply to all members of the subclasses.
Isolation
Subclass
133.
Plaintiffs Gamez, Swartz, Brislan, Rodriguez, Verduzco, Thomas,
Smith, and Polson bring this action on their own behalf and, pursuant
to Rules 23(a), 23(b)(1), and 23(b)(2) of the Federal Rules of Civil
Procedure, against Defendants Ryan and Pratt on behalf of a subclass
of all prisoners (hereinafter “Isolation Subclass”) who are now,
or will in the future be, subject by the ADC to isolation, defined as
confinement in a cell for 22 hours or more each day or confinement in
Eyman - SMU 1, Eyman - Browning Unit,
Florence
- Central Unit, or Perryville - Lumley Unit Special Management Area
(SMA).
Numerosity:
Fed. R. Civ. P. 23(a)(1)
134.
The Isolation Subclass is so numerous that joinder of all members is
impracticable. Each year approximately 3,000 prisoners are subjected
to Defendants’ policies and practices of denying minimally adequate
conditions of confinement while in isolation. The Isolation Subclass
members are identifiable using records maintained in the ordinary
course of business by the ADC.
Commonality:
Fed. R. Civ. P. 23(a)(2)
135.
There are questions of law and fact common to the members of the
Isolation Subclass. Such questions include, but are not limited to:
(a)
whether Defendants’ policy and practice of not providing a housing
environment free of debilitating isolation and inhumane conditions to
prisoners subjected to isolation violates the Cruel and Unusual
Punishments Clause of the Eighth Amendment,
(b)
whether Defendants have been deliberately indifferent to the
Isolation Subclass members’ risk of injury and harm from the
debilitating isolation and inhumane conditions to which they are
subjected.
Defendants
are expected to raise common defenses to these claims, including
denying that their actions violated the law.
Typicality:
Fed. R. Civ. P. 23(a)(3)
136.
The claims of the Plaintiffs are typical of those of the Isolation
Subclass, because their claims arise from the same policies,
practices, or courses of conduct; and their claims are based on the
same theory of law as the subclass’s claims.
Adequacy:
Fed. R. Civ. P. 23(a)(4)
137.
Plaintiffs are capable of fairly and adequately protecting the
interests of the Isolation Subclass because Plaintiffs do not have
any interests antagonistic to the subclass. Plaintiffs, as well as
the Isolation Subclass members, seek to enjoin the unlawful acts and
omissions of Defendants. Finally, Plaintiffs are represented by
counsel experienced in civil rights litigation, prisoners’ rights
litigation, and complex class action litigation.
Fed.
R. Civ. P. 23(b)(1)(A) and (B)
138.
Since the number of Isolation Subclass members is approximately
3,000, the prosecution of separate actions by individuals would
create a risk of inconsistent and varying adjudications, which in
turn would establish incompatible standards of conduct for Defendants
Ryan and Pratt. Additionally, the prosecution of separate actions by
individual members could result in adjudications with respect to
individual members that, as a practical matter, would substantially
impair the ability of other members to protect their interests.
Fed.
R. Civ. P. 23(b)(2)
139.
Defendants’ policies, practices, actions, and omissions that form
the basis of the claims of the Isolation Subclass are common to and
apply generally to all members of the subclass, and the injunctive
and declaratory relief sought is appropriate and will apply to all
members of the subclass. All state-wide policies on the conditions of
isolation are centrally promulgated, disseminated, and enforced from
the central headquarters of ADC by Defendants Ryan and Pratt. The
injunctive and declaratory relief sought is appropriate and will
apply to all members of the subclass.
CLAIMS
FOR RELIEF
First
Cause of Action
(All
Prisoner Plaintiffs and the Plaintiff Class v. Defendants Ryan and
Pratt)
(42
U.S.C. § 1983; Eighth Amendment)
140.
By their policies and practices described herein, Defendants subject
all prisoner Plaintiffs and the Plaintiff class to a substantial risk
of serious harm and injury from inadequate health care. These
policies and practices have been and continue to be implemented by
Defendants and their agents, officials, employees, and all persons
acting in concert with them under color of state law, in their
official capacities, and are the proximate cause of the Plaintiffs’
and the Plaintiff Class’s ongoing deprivation of rights secured by
the United States Constitution under the Eighth Amendment.
141.
Defendants have been and are aware of all of the deprivations
complained of herein, and have condoned or been deliberately
indifferent to such conduct.
Second
Cause of Action
(Plaintiffs
Jensen, Swartz, Chisholm, Licci, Hefner, Polson, and Wells; and
Medical Subclass v. Defendants Ryan and Pratt)
(42
U.S.C. § 1983; Eighth Amendment)
142.
By their policies and practices described herein, Defendants subject
Plaintiffs Jensen, Swartz, Chisholm, Licci, Hefner, Polson, and
Wells, and the Medical Subclass to a substantial risk of serious harm
and injury from inadequate medical care. These policies and practices
have been and continue to be implemented by Defendants and their
agents, officials, employees, and all persons acting in concert with
them under color of state law, in their official capacities, and are
the proximate cause of the Plaintiffs’
and
the Medical Subclass’s ongoing deprivation of rights secured by the
United States Constitution under the Eighth Amendment.
143.
Defendants have been and are aware of all of the deprivations
complained of herein, and have condoned or been deliberately
indifferent to such conduct.
///
Third
Cause of Action
(Plaintiffs
Swartz, Parsons, Chisholm, Polson, and Wells; and Dental Subclass v.
Defendants Ryan and Pratt)
(42
U.S.C. § 1983; Eighth Amendment)
144.
By their policies and practices described herein, Defendants subject
Plaintiffs Swartz, Parsons, Chisholm, Polson, and Wells, and the
Dental Subclass to a substantial risk of serious harm and injury from
inadequate dental care. These policies and practices have been and
continue to be implemented by Defendants and their agents, officials,
employees, and all persons acting in concert with them under color of
state law, in their official capacities, and are the proximate cause
of the Plaintiffs’ and the Dental Subclass’s ongoing deprivation
of rights secured by the United States Constitution under the Eighth
Amendment.
145.
Defendants have been and are aware of all of the deprivations
complained of herein, and have condoned or been deliberately
indifferent to such conduct.
Fourth
Cause of Action
(Plaintiffs
Gamez, Swartz, Brislan, Rodriguez, Verduzco, Thomas, Smith, Parsons,
Chisholm, and Polson; Plaintiff Arizona Center for Disability Law;
and Mental Health Subclass v. Defendants Ryan and Pratt)
(42
U.S.C. § 1983; Eighth Amendment)
146.
By their policies and practices described herein, Defendants subject
Plaintiffs
Gamez, Swartz, Brislan, Rodriguez, Verduzco, Thomas, Smith, Parsons,
Chisholm, and Polson, and the Mental Health Subclass to a substantial
risk of serious harm and injury from inadequate mental health care.
These policies and practices have been and continue to be implemented
by Defendants and their agents, officials, employees, and all persons
acting in concert with them under color of state law, in their
official capacities, and are the proximate cause of the Plaintiffs’
and the Mental Health Subclass’s ongoing deprivation of rights
secured by the United States Constitution under the Eighth Amendment.
147.
Defendants have been and are aware of all of the deprivations
complained of herein, and have condoned or been deliberately
indifferent to such conduct.
Fifth
Cause of Action
(Plaintiffs
Gamez, Swartz, Brislan, Rodriguez, Verduzco, Thomas, Smith, and
Polson; and Plaintiff Arizona Center for Disability Law; and
Isolation Subclass v. Defendants Ryan and Pratt)
(42
U.S.C. § 1983; Eighth Amendment)
148.
By their policies and practices described herein, Defendants subject
Plaintiffs Gamez, Swartz, Brislan, Rodriguez, Verduzco, Thomas,
Smith, and Polson, and the Isolation Subclass to a substantial risk
of serious harm and injury from inadequate physical exercise,
inadequate nutrition, inadequate mental health treatment, and
conditions of extreme social isolation and environmental deprivation.
These policies and practices have been and continue to be implemented
by Defendants and their agents, officials, employees, and all persons
acting in concert with them under color of state law, in their
official capacities, and are the proximate cause of the Plaintiffs’
and the Isolation
Subclass’s
ongoing deprivation of rights secured by the United States
Constitution under the Eighth Amendment.
149.
Defendants have been and are aware of all of the deprivations
complained of herein, and have condoned or been deliberately
indifferent to such conduct.
///
PRAYER
FOR RELIEF
150.
Plaintiffs and the classes they represent have no adequate remedy at
law to redress the wrongs suffered as set forth in this complaint.
Plaintiffs have suffered and will continue to suffer irreparable
injury as a result of the unlawful acts, omissions, policies, and
practices of Defendants Ryan and Pratt, as alleged herein, unless
Plaintiffs and the classes they represent are granted the relief they
request. The need for relief is critical because the rights at issue
are paramount under the United States Constitution and the laws of
the United States.
151.
WHEREFORE, the named plaintiffs and the classes they represent
request that this Court grant them the following relief:
A.
Declare that the suit is maintainable as a class action pursuant to
Federal Rule of Civil Procedure 23(a) and 23(b)(1) and (2);
B.
Adjudge and declare that the acts, omissions, policies, and practices
of Defendants, and their agents, employees, officials, and all
persons acting in concert with them under color of state law or
otherwise, described herein are in violation of the rights of
prisoner Plaintiffs and the classes they represent under the Cruel
and Unusual
Punishments
Clause of the Eighth Amendment, which grants constitutional
protection to the Plaintiffs and the class they represent;
C.
Preliminarily and permanently enjoin Defendants, their agents,
employees, officials, and all persons acting in concert with them
under color of state law, from subjecting prisoner Plaintiffs and the
Plaintiff Class to the illegal and unconstitutional conditions, acts,
omissions, policies, and practices set forth above.
D.
Order Defendants and their agents, employees, officials, and all
persons acting in concert with them under color of state law, to
develop and implement, as soon as practical, a plan to eliminate the
substantial risk of serious harm that prisoner Plaintiffs and members
of the Plaintiff Class suffer due to Defendants’ inadequate
medical, mental health, and dental care, and due to Defendants’
isolation policies. Defendants’ plan shall include at a minimum the
following:
1.
Staffing: Staffing shall be sufficient to provide prisoner Plaintiffs
and the Plaintiff Class with timely access to qualified and competent
clinicians who can provide routine, urgent, emergent, and specialty
health care;
2.
Access: Policies and practices that provide timely access to health
care;
3.
Screening: Policies and practices that reliably screen for medical,
dental, and mental health conditions that need treatment;
4.
Emergency Response: Timely and competent responses to health care
emergencies;
5.
Medication and Supplies: Timely prescription and distribution of
medications and supplies necessary for medically adequate care;
6.
Chronic Care: Timely access to competent care for chronic diseases;
7.
Environmental Conditions: Basic sanitary conditions that do not
promote the spread or exacerbation of diseases or infections,
including but not limited to a smoke-free environment;
8.
Mental Health Treatment: Timely access to necessary treatment for
serious mental illness, including medication, therapy, inpatient
treatment, suicide prevention, and suicide watch;
9.
Quality Assurance: A regular assessment of health care staff,
services, procedures, and activities designed to improve outcomes,
and to identify and correct errors or systemic deficiencies;
10.
Isolation: Prohibition of confinement of prisoner Plaintiffs and the
Isolation Subclass under conditions of social isolation and sensory
deprivation that put prisoners at substantial risk of serious
physical and mental harm. Providing prisoner Plaintiffs and the
Isolation Subclass with necessary nutrition and regular outdoor
exercise to preserve their physical and mental health.
E.
Award Plaintiffs the costs of this suit, and reasonable attorneys’
fees and litigation expenses pursuant to 42 U.S.C. § 1988, and other
applicable law;
F.
Retain jurisdiction of this case until Defendants have fully complied
with the orders of this Court, and there is a reasonable assurance
that Defendants will continue to comply in the future absent
continuing jurisdiction; and
G.
Award such other and further relief as the Court deems just and
proper.
Dated:
March 22, 2012
ACLU
FOUNDATION OF ARIZONA
By:
/s/ Daniel J. Pochoda
Daniel
J. Pochoda
James
Duff Lyall
Donald
Specter (Cal. 83925)*
Alison
Hardy (Cal. 135966)*
Sara
Norman (Cal. 189536)*
Corene
Kendrick (Cal. 226642)*
PRISON
LAW OFFICE
1917
Fifth Street
Berkeley,
CA 94710
Telephone:
(510) 280-2621
*Application
for pro hac vice pending
David
C. Fathi (Wash. 24893)*
Amy
Fettig (D.C. 484883) *
ACLU
NATIONAL PRISON PROJECT
915
15th St. N.W., 7th Floor
Washington,
D.C. 20005
Telephone:
(202) 548-6603
*Application
for pro hac vice pending
Daniel
C. Barr (SBA 010149)
Jill
L. Ripke (SBA 024837)
James
A. Ahlers (SBA 026660)
Kirstin
T. Eidenbach (SBA 027341)
John
H. Gray (SBA 028107)
Thomas
D. Ryerson (SBA 028073)
Matthew
B. Du Mée (SBA 028468)
PERKINS
COIE LLP
2901
N. Central Ave., Suite 2000
Phoenix,
AZ 85012-2788
Telephone:
(602) 351-8000
dbarr@perkinscoie.com
jripke@perkinscoie.com
jahlers@perkinscoie.com
keidenbach@perkinscoie.com
jhgray@perkinscoie.com
tryerson@perkinscoie.com
mdumee@perkinscoie.com
Caroline
Mitchell (Cal. 143124)*
Douglas
Roberts (Cal. 264451)*
JONES
DAY
555
California St., 26th Floor
San
Francisco, CA 94104
Telephone:
(415) 875-5712
cnmitchell@jonesday.com
*Application
for pro hac vice pending
Attorneys
for Plaintiffs Victor Parsons, Shawn Jensen, Stephen Swartz, Dustin
Brislan, Sonia Rodriguez, Christina Verduzco, Jackie Thomas, Jeremy
Smith, Robert Gamez, Maryanne Chisholm, Desiree Licci, Joseph Hefner,
Joshua Polson, and Charlotte Wells, on behalf of themselves and all
others similarly situated
ARIZONA
CENTER FOR DISABILITY LAW
By:
/s/ Jennifer Alewelt
Jennifer
Alewelt (SBA 027366)
Ruth
Szanto (SBA 029073)
5025
East Washington St. Suite 202
Phoenix,
AZ 85034
Telephone
(602) 274-6287
jalewelt@azdisabilitylaw.org
rszanto@azdisabilitylaw.org
Attorneys
for Plaintiff Arizona Center for Disability Law
CERTIFICATE
OF SERVICE
I
hereby certify that on March 22, 2012, I electronically transmitted
the attached documents to the Clerk’s Office using the CM/ECF
System.
/s/
Gloria Torres
Case
2:12-cv-00601-NVW--MEA Document 1 Filed 03/22/12
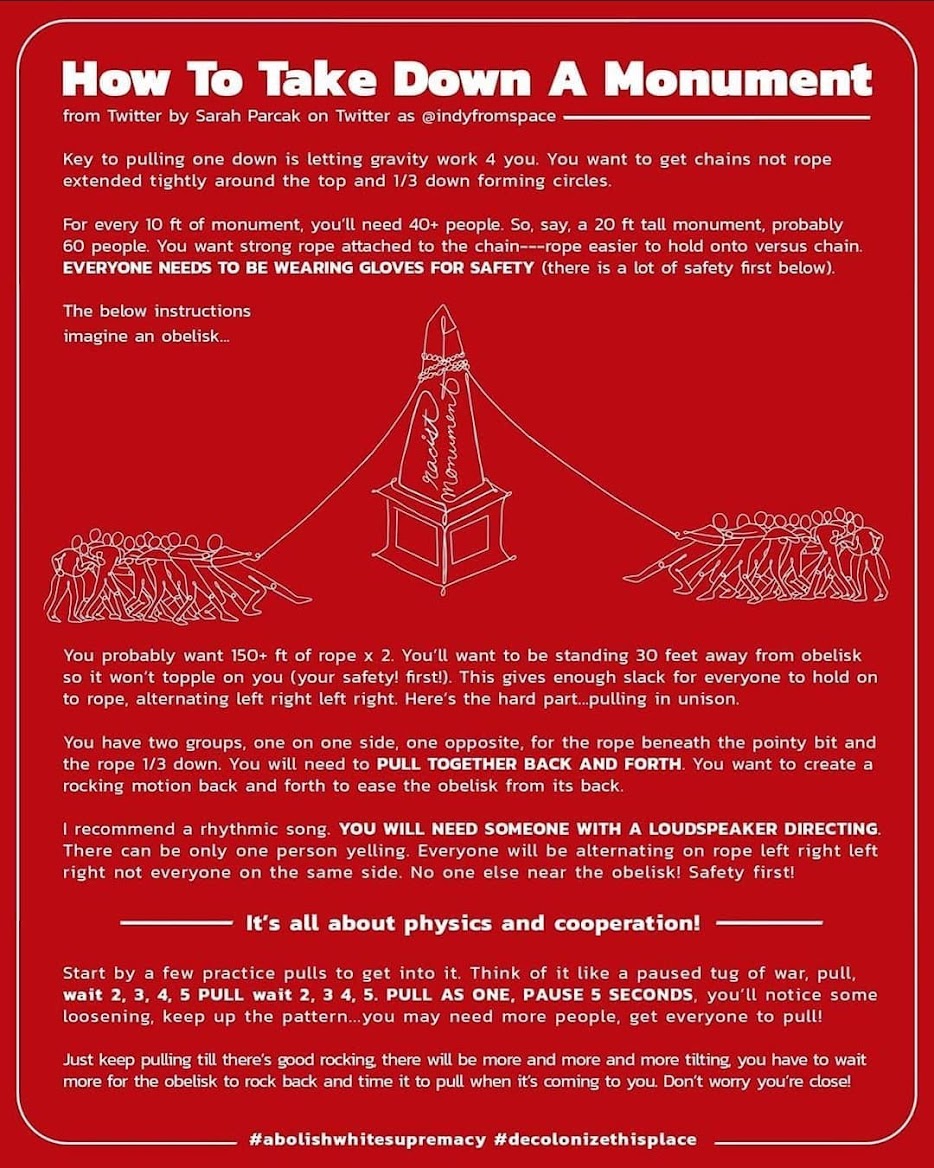














.jpg)





.JPG)
































1.jpg)






{kind=link}
{kind=link}